


Source: National Institutes of Health / NIAID / Science Photo Library
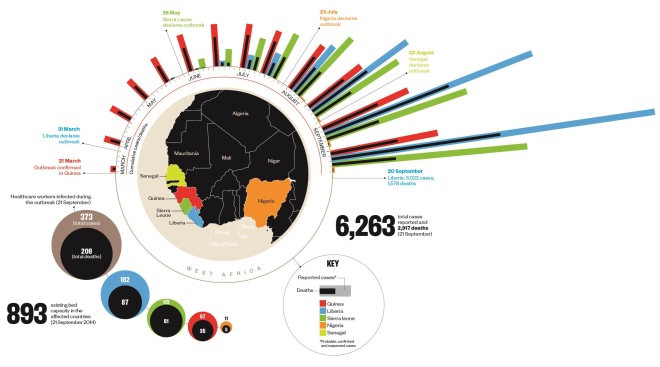
Timeline
Six months into the outbreak and the virus has spread to five countries in West Africa. Although cases in Nigeria, Senegal and Guinea appear to have stabilised, cases in Liberia and Sierra Leone continue to rise.
Transmission and symptoms
Ebola virus enters the patient through mucous membranes, broken skin, or parenterally. The virus exerts its effects directly, by causing cell necrosis, and indirectly, by causing apoptosis (programmed cell death). Apoptosis is prompted by the release of cytokines from infected cells. The virus infects many cell types, including monocytes, macrophages, dendritic cells, endothelial cells, fibroblasts, hepatocytes, adrenal cortical cells and epithelial cells. Although lymphocytes are not infected, they undergo apoptosis.
![]()
![]()
A) Fever, headache and chills are caused by the host mounting an overt immune (cytokine) response to the Ebola virus.
B) Bleeding from the eyes, ears and mouth is caused by loss of vascular integrity due to endothelial cell death and dysregulation of clotting factors because of hepatocellular necrosis.
C) Impaired kidney and liver function is caused by death of renal and hepatic cells infected by the virus; there may also be some level of apoptosis in these tissues.
D) The virus evades the immune response by causing rapid destruction of lymphoid tissue, including B and T cells, and disrupting the interferon response.
E) Severe watery diarrhoea, nausea, vomiting and abdominal pain is likely to be caused by necrotic infection of the gastrointestinal tract, resulting in loss of the ciliated cells required for absorption of nutrients. The physical damage leads to gastrointestinal bleeding and the other gastrointestinal symptoms.
F) Muscle pain and weakness is likely to be due to the host immune (cytokine) response to the virus.
G) Haemorrhagic rash over the entire body, bruising, and oozing from venipuncture sites is caused by loss of vascular integrity due to endothelial cell death and dysregulation of clotting factors because of hepatocellular necrosis.
The biology
Ebola virus attaches to the cell surface and is internalised, subsequently releasing its genetic material into the host cell cytoplasm. The RNA genome of the virus is transcribed into seven mRNAs, which are translated into the viral proteins. Some of these proteins then aid replication of the viral genome while others are destined to become the viral coating. New viral particles are then assembled from the replicated genome and new coat proteins and these bud from the cell.
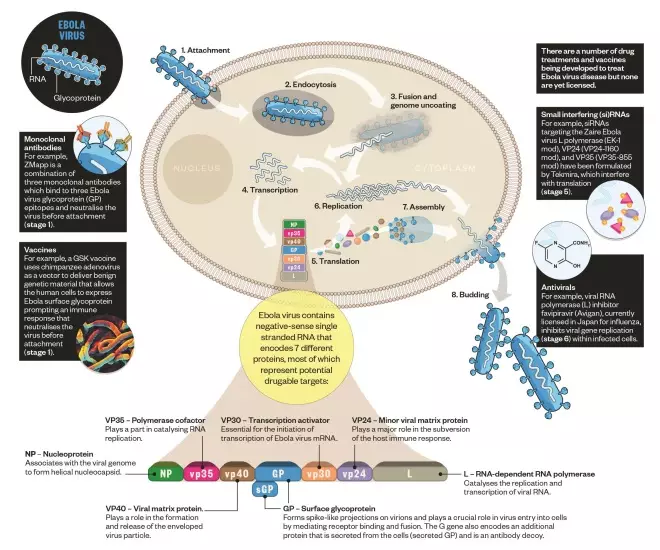
Biology of the Ebola virus
Country characteristics
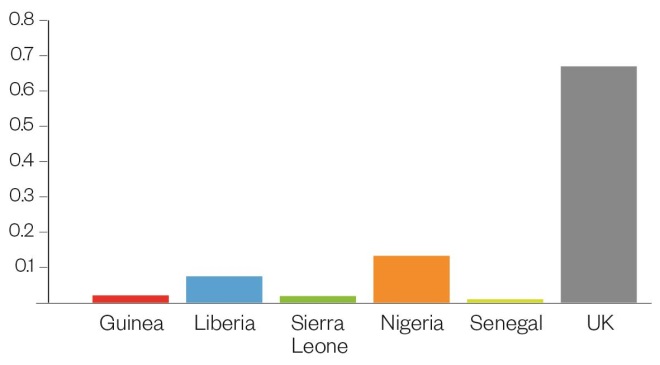
The West African countries worst affected by the outbreak have poorly developed health systems, with little public health infrastructure and few healthcare professionals. The last bar in each chart allows comparison with the UK.
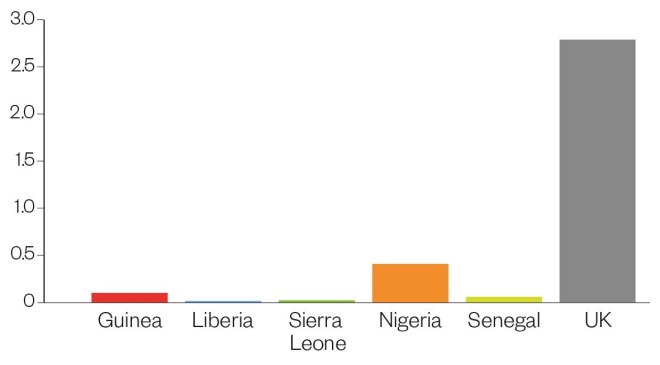
Doctors per 1,000 population. Liberia has the lowest density of doctors at just 1 in 71,429 of the population.
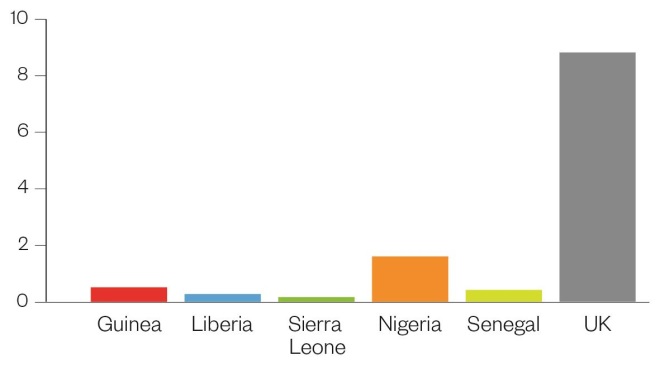
Nurses and midwives per 1,000 population. Sierra Leone has the lowest number of nurses and midwives, at 1 for every 6,024 people.
Pharmaceutical personnel per 1,000 population. Senegal has only one pharmacy worker for every 100,000 people.
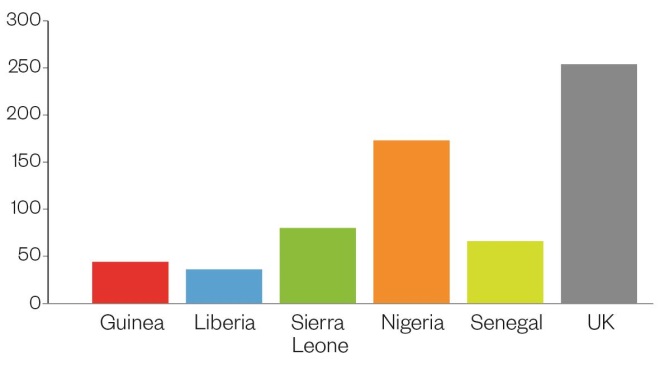
Population density per square kilometre. Nigeria has the highest population density of countries affected but also by far the highest density of medical professionals.
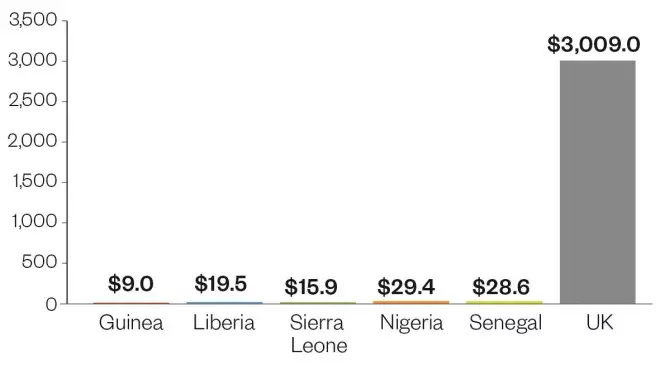
Government expenditure on health per capita ($US). The combined per capita spend of the affected countries is less than 4% of that of the UK.


