A 65-year-old man was admitted with a six-day history of intermittent high fever, malaise and a poor appetite. He had a brief period of acute confusion on the day before admission. There was no recent history of dental work or surgery. His past medical history included a myocardial infarction in 2004, congestive cardiac failure, hypertension and a heart murmur corresponding to mitral regurgitation. His regular medicines included:
- Aspirin 75mg od;
- Furosemide 40mg od;
- Simvastatin 40mg od;
- Ramipril 5mg od;
- Bisoprolol 2.5mg od;
- Omeprazole 40mg od;
- Paracetamol 1g qds.
He was documented to have a penicillin allergy producing a rash as a child. The patient, a retired plastics engineer, had never smoked or engaged in intravenous drug use. On examination, he appeared acutely ill. His body temperature was 39.2C, blood pressure was 105/75mmHg, pulse rate was 110 beats/min, and respiratory rate was 24 breaths/min. On listening to his heart, a loud murmur could be heard. His spleen was palpably enlarged, and he had a generalised erythematous macular non-blanching skin rash, especially on his palms and soles (Janeway lesions; see Box below).

Box: Infective endocarditis: background knowledge
Infective endocarditis is an endovascular infection of cardiovascular structures, including heart valves. Annual incidence in the UK is six to seven per 100,0001. Without treatment mortality approaches 100%. Even with treatment mortality and morbidity are significant. Endocarditis is usually the consequence of two factors: the presence of bacteria in the bloodstream and abnormal cardiac endothelium promoting their adherence and growth. The commonest bacterium implicated in causing endocarditis is Streptococcus viridans2. Physicians should suspect endocarditis inpatients with:
- A new heart murmur;
- An embolic event of unknown origin;
- Sepsis of unknown origin;
- Haematuria, glomerulonephritis and suspected renal infarction;
- Fever plus prosthetic material inside the heart; risk factors for bacteraemia (ie, iv drug use, recent dental work or surgical procedure);positive blood cultures with typical organisms for endocarditis; cutaneous signs (Osler nodes (see main text) and Janeway lesions — haemorrhagic macular or nodular lesions on the palms or soles) or peripheral abscesses (renal, splenic, spine) of unknown origin2.
Investigations are required to confirm the diagnosis and to monitor the patient’s response to therapy including1:
- Blood cultures (three sets taken at different times and different sites at peak fever);
- Blood tests (for detecting anaemia, neutrophilia, high inflammatory markers, such as C-reactive protein and erythrocyte sedimentation rate; renal and liver function);
- Urinalysis (will reveal microscopic haematuria);
- Electrocardiogram (may show conduction defects);
- Chest X-ray (may show evidence of pulmonary abscesses or heart failure);
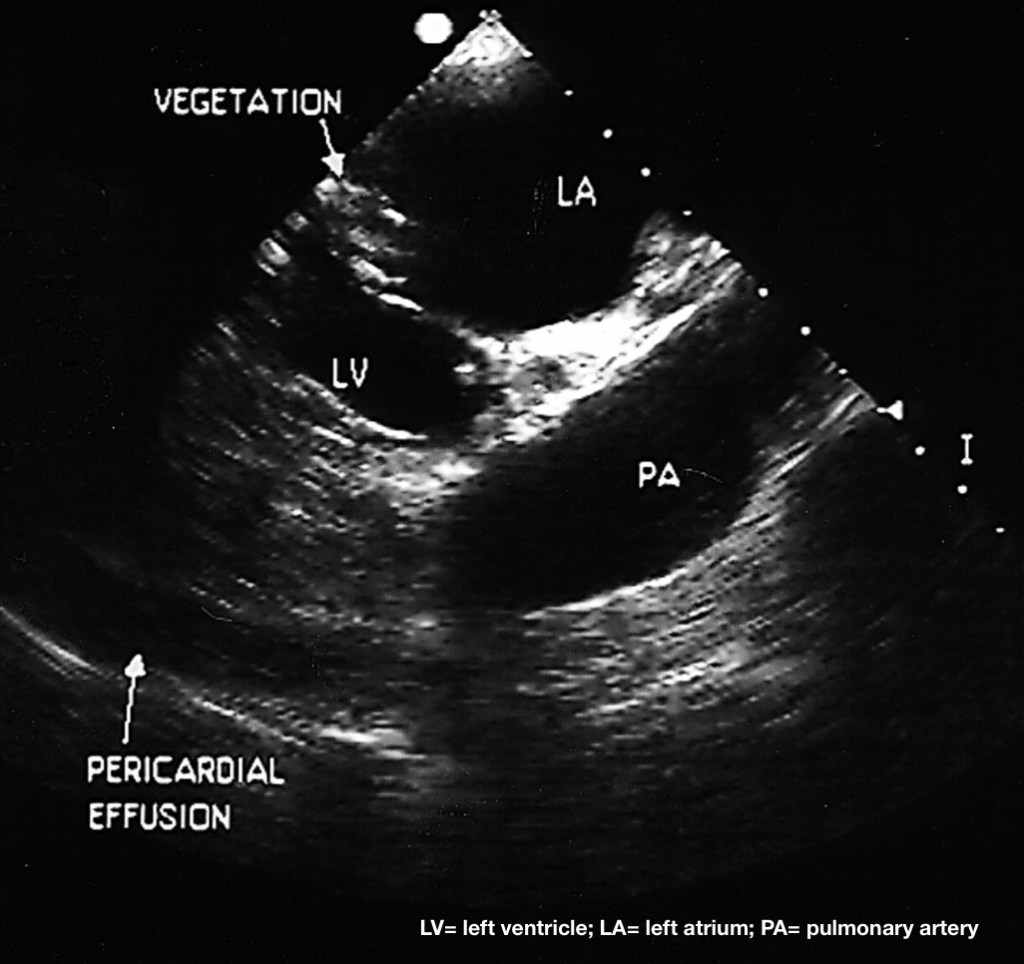
- Echocardiography (may reveal vegetation and other complications).
The location of the infection means that prolonged courses of antibiotics are usually required intravenously for four to six weeks. Advice on therapy should be sought from a microbiologist, according to the organism identified and current sensitivities. Surgical interventions are considered if there are features of heart failure, myocardial abscess or unstable infected prosthetic valve1,2.
The value of antibiotic prophylaxis for invasive diagnostic, dental or surgical procedures has never been established in randomised controlled trials, so their widespread use has been questioned. Recent National Institute for Health and Clinical Excellence guidelines suggest no prophylaxis unless there is an infection at the site of gastrointestinal or genitourinary tract procedures in patients at risk of endocarditis — the adverse effects of antibiotics outweigh the risks3.
Laboratory results
Initial laboratory results revealed a white cell count of 19.8×109/L with neutrophilia. C-reactive protein was 292mg/L. The patient’s renal and liver profiles were normal. Urinalysis was positive for blood (+++) and protein (+). Chest X-ray was normal. An echocardiogram performed on the day of admission (see left) revealed mitral valve vegetation with severe mitral regurgitation and normal ejection fraction. At this stage infective endocarditis was suspected and empirical intravenous gentamicin 300mg od and vancomycin 500mg bd started.
On day three, the patients’ general condition deteriorated. He became drowsy, breathless and oliguric, and displayed slurred speech with right-sided arm and leg weakness. His renal function worsened acutely from a baseline serum creatinine of 75μmol/L to378μmol/L on day 4. His liver function was also acutely deranged, with bilirubin 62μmol/L, alanine amino transferase 745iu/Land alkaline phosphatase 412iu/L.
A subsequent CT (computed tomography) scan of the brain was normal, but an MRI (magnetic resonance imaging) scan identified multiple areas of white matter abnormality suggestive of embolism around the periventricular area. Two sets of blood cultures taken at admission subsequently grew Staphylococcus aureus sensitive to gentamicin, flucloxacillin, rifampicin and vancomycin.
Case comment — Helen Williams, consultant pharmacist for cardiovascular disease, south London
This case highlights many of the challenges in treating patients with infective endocarditis. Targeted and well managed antibiotic therapy is the key to successful treatment. Early identification of the causative organism is, therefore, essential. As in this case, blood cultures should be drawn before the initiation of empirical antibiotic therapy — early antibiotic exposure before drawing blood cultures is the most common reason for a culture negative result, which leaves clinicians unsure of the specific bacteria responsible and prevents tailored antibiotic therapy in accordance with sensitivities.
Antibiotic regimen
Delivering the antibiotic regimen at an appropriate dose and frequency is the next challenge. Bacteria form bio-films on the endothelial surface which prevent penetration of antibiotics and therefore reduce treatment efficacy, resulting in the need for high doses for prolonged periods.

High-dose beta-lactam antibiotic therapy is the usual mainstay of treatment, but penicillin allergy precluded this approach here.
Different dosing strategies are required for different antibiotic classes — penicillins need to maintain a minimum inhibitory concentration throughout the 24 hours so are often therefore given at high doses six times a day. In contrast, the efficacy of aminoglycosides is related to achieving a specific peak level, while toxicity occurs where there is failure to achieve adequate trough levels — careful monitoring and adjustment of dose and frequency in response to changes in renal function with the aim of maximising efficacy and minimising risk is essential. This can be a fine balance, particularly in a condition where, without adequate treatment, mortality is nearing 100%. In some patients achieving adequate antibiotic doses to maximise efficacy will lead to toxic effects, which may have to be accepted as inevitable and dealt with when they occur.
Surgery
The timing of surgery inpatients with infective endocarditisis also a critical issue. Early surgerymay be justifiable in patients withacute decompensated heart failure,where antibiotic therapy has failedto control the infection, and wherethere is a need to prevent furtherembolic events. However, delaying surgery, as in this case, allows medical treatment of the infection, which in turn improves surgical success rates and reduces the likelihood of infection of the implanted prosthetic valve.
Guidelines
The author of this case report also mentions the role of antibiotic prophylaxis in patients at risk of infective endocarditis who are undergoing dental procedures or surgery. The NICE guidance has taken a unique position in recommending that no antibiotic prophylaxis should be given to patients with a newly implanted prosthetic valve. This has proved a controversial recommendation, stimulating heated debate between heart surgeons and microbiologists. European and American guidelines published since the NICE guidance do support the use of antibiotic prophylaxis in specified high risk groups, including patients with prosthetic valves.
Diagnosis
A diagnosis of “Staphylococcus aureus infective endocarditis” was made. It was thought the patient was now beginning to display complications of endocarditis, namely:
- Valve destruction causing decompensated heart failure
- Embolic phenomena (“showering” of septic particles from the heart lesion causing extracardiac abscess formation, ischaemic stroke and renal infarcts)
- Immune complex deposition (antibody-antigen binding with subsequent systemic deposition causing inflammation [eg, in the kidneys producing glomerulonephritis and then renal failure] splinter haemorrhages on finger and toe nails, Osler’s nodes [painful pulp infarcts in fingers and toes] and, eventually, multi-organ failure).
Treatment
The patient was transferred to the intensive care unit and several professionals were summoned, each contributing to optimise care. In view of the culture report, the resident microbiologist suggested antibiotics were continued but with the doses adjusted (previous doses were subtherapeutic) and regular monitoring as follows:
• Gentamicin 120mg iv eight-hourly; drug levels every three days (troughs should be ≤2 and peaks 4–8mg/L)
• Vancomycin 1g iv 12-hourly; drug levels every three days (troughs should be 10–15 and peaks 30–45mg/L).
Pharmacists were closely involved with monitoring and adjusting the iv antibiotic doses to ensure levels were neither toxic nor subtherapeutic. As the patient developed acute renal and liver impairment, doses of regular medicines were adjusted. Simvastatin and paracetamol were withheld due to the impairment in hepatic function.
The pharmacist also organised paracetamol levels to be determined, in view of regular paracetamol ingestion during the acute deterioration in liver function. These were found to be as high as 20mg/L, suggesting paracetamol had accumulated, and the patient was given acetylcysteine. The dose of omeprazole was reduced to 20mg od because of liver impairment. Ramipril was withheld because of acute renal impairment.
The gentamicin and vancomycin doses were adjusted to 80mg od and 500mg od, respectively, guided by serum antibiotic levels. Total parenteral nutrition was organised (via the pharmacy) while the patient’s swallow was deemed unsafe and until nasogastric feeding could be established. The patient’s tablets were switched to liquid formulations where possible.
Once antibiotic therapy was optimised, the patient became afebrile on day five. His rashes started to fade and his right-sided weakness began to resolve. His renal and liver function improved sufficiently to discontinue the haemofiltration started on day three. Two weeks later, gentamicin was substituted for rifampicin 600mg po bd. This, together with vancomycin, was continued for six weeks. In week eight, the patient underwent a successful metallic mitral valve replacement and was started on warfarin. He was discharged three months later on the following medicines:
- Warfarin (effects enhanced by statin use so GP advised to monitor INR [international normalised ratio] closely);
- Furosemide 80mg od;
- Simvastatin 40mg od;
- Ramipril 2.5mg od;
- Omeprazole 20mg od.
Role of the pharmacist
This case highlights the pivotal role of the pharmacist in ensuring patients receive optimal drug therapy. Monitoring was essential and pharmacists were ideally placed to ensure drug levels are neither subtherapeutic nor toxic.
As the patient’s condition deteriorated pharmacists were closely involved in discontinuing drugs, suggesting alternatives or adjusting doses of medicines that might have adverse effects in renal or hepatic impairment. Pharmacists also have a role in counselling patients starting long-term therapy, such as warfarin.
Share your cases
Readers with interesting clinical cases to share are invited to contact Lin-NamWang
- 1.Beynon RP, Bahl VK, Prendergast BD. Infective endocarditis. BMJ. 2006;333(7563):334-339. doi:10.1136/bmj.333.7563.334
- 2.Wilkinson I, Turmezei T, Smith E, Cheung C, Longmore M. Oxford Handbook of Clinical Medicine. 7th ed. Oxford University ; 2007.
- 3.Prophylaxis against infective endocarditis: antimicrobial prophylaxis against infective endocarditis in adults and children undergoing interventional procedures. The National Institute for Health and Care Excellence . March 2008. https://www.nice.org.uk/guidance/cg64