


Shutterstock.com
Adequate hydration is essential for the human body to maintain organ perfusion and cell metabolism. Inadequate fluid intake and excessive fluid loss can lead to both dehydration, which can affect heart and kidney function, and problems with electrolyte management. Many adult hospital inpatients require intravenous (IV) fluid therapy to prevent or correct problems with their fluid and/or electrolyte status. However, deciding on the optimal dose and composition of IV fluids, as well as the rate at which to give them, can be very complex[1]
. Pharmacists understand the supply chain, are aware of the different fluid solutions available and know of the practice and maths of dilution, meaning they are suitably placed to deliver the care that patients require.
The evidence base supporting optimal or best practice in this area is poor; while there are many studies on fluid management, they usually include small numbers of around 20–50 patients within a specific cohort (e.g. post-pancreatic surgery). Furthermore, randomised, double-blind, placebo-controlled trials of large numbers (over 5,000 patients) are rare. The only large-scale randomised-controlled trial was the Saline versus Albumin Fluid Evaluation study (known as the ‘SAFE’ study) in Australia and New Zealand in 2004 that compared albumin with saline[2]
. Owing to the dearth of evidence, the National Institute for Health and Care Excellence (NICE) developed guidance on IV fluid therapy for general areas of hospital practice, covering both the prescription and monitoring of IV fluid and electrolyte therapy in patients aged 16 years and over[1]
.
This article provides an introduction to fluid management; the physiology that supports the rationale for prescribing IV fluids; the impact of vasodilatation and vasoconstriction; and the role of the pharmacist in managing patients. This article will not cover hypovolaemia with hypernatraemia or colloids (because the data are both complex and controversial). Interested readers are instead referred to the crystalloid/colloid debate that has continued for more than two decades[3],[4]
.
Basic physiological principles of fluid therapy
Healthy individuals gain fluids from their food and drink intake, and predominately lose them via urine, sweat and faeces. Around 60% of total body weight is water, although this does vary between individuals owing to age, sex and amount of fat stored in the body[5]
. Water is distributed in the body in fluid compartments: the intracellular fluid compartment (around 40% of body weight) and extracellular fluid compartment (around 20% of body weight; see Figure 1). The extracellular fluid compartment comprises the vascular compartment (blood vessels) and the interstitial space (the gaps between the cells).
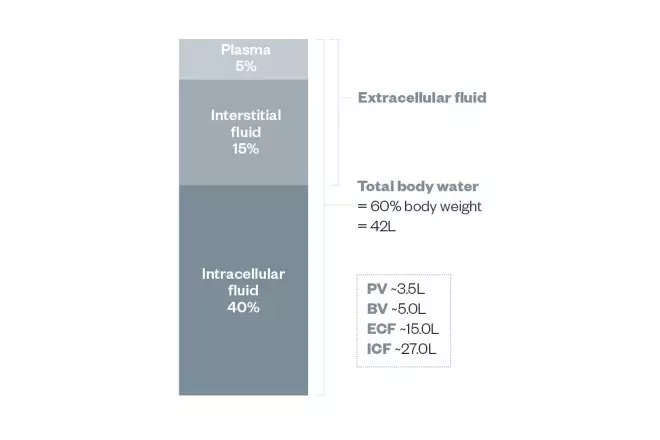
Figure 1: Fluid compartments
Source: Mark Tomlin
The fluid compartments of the human body, by percentage of mass (total body weight)
Water can move freely across the membranes that separate the compartments to maintain osmotic equilibrium. Osmotically active substances — predominantly albumin and sodium — bind water in the intravascular compartment and thereby ensure that the circulating blood volume is adequate. Fluids are normally administered into the plasma where they can be removed via the kidneys. Water and electrolytes then move out to the interstitial spaces.
Fluid and electrolyte composition
Body water contains electrolytes, such as sodium (Na+), potassium (K+), chloride (Cl–), bicarbonate (HCO3–), calcium (Ca2+) and magnesium (Mg2+) (see Table 1).
Table 1: Electrolyte composition of body compartments | |||
| Plasma cations (mmol/L) | Plasma anions (mmol/L) | Intracellular cations (mmol/L) | Intracellular anions (mmol/L) |
| Na+ 140 | Cl– 108 | K+ 157 | PO43– 113 |
| K+ 5 | HCO3– 27 | Mg2+ 26 | Protein– 74 |
| Ca2+ 2.3 | Protein– 16 | Na+ 14 | HCO3– 10 |
| Mg2+ 0.7 | |||
| Source: Adapted from Chapter 4: The heart and circulation. In An introduction to Human Physiology 4th Ed. 1976. JH Green Oxford Medical Publications 7 | |||
Movement of fluids
Fluid and electrolyte levels in the body are kept relatively constant by several complex homeostatic mechanisms. Electrolytes move by diffusion from an area of high concentration to an area of low concentration. The body uses the energy from metabolising carbohydrates and fats to generate adenosine triphosphate (ATP), which then drives electrolyte pumps[6]
. Therefore, electrolytes and their volume in the plasma are regulated by the Na+/K+ ATPase pump. However, it should also be noted that the presence of albumin in the plasma also exerts a colloid osmotic force, holding water in the plasma.
Insulin moves glucose into body tissues and carries electrolytes with it. As a result, administering IV glucose to a patient who does not have diabetes will move potassium (and other electrolytes) into the tissues.
Organ perfusion
The perfusion of the body via blood is principally determined by systemic blood flow (cardiac output). However, venous return, vascular tone (the degree of constriction experienced by a blood vessel) and plasma volume are major factors; maximum cardiac output is limited by venous return. Increasing the vascular tone (i.e. constricting the blood vessels) reduces the cross-sectional area of the blood vessels, increasing the resistance to blood flow[7]
.
Where plasma volume is inadequate to fill the blood vessel capacity, blood pressure will be low and could represent extreme dehydration and hypovolaemia. In this situation, the body adapts by secreting adrenaline, which causes constriction of the blood vessels and makes the plasma volume appear to rise (although the actual volume remains the same) and increases blood pressure to allow for adequate perfusion of vital organs. Thus, adrenaline can also be described as a vasopressor. When the vascular smooth muscle relaxes and the lumen of the blood vessel expands, the blood pressure falls and the patient could be described as relatively hypovolaemic (although the actual volume has not changed).
Good fluid management should occur before the use of pharmacological vasoconstrictors[8]
.
Pathophysiology
Systemic blood pressure is maintained by plasma volume and vascular tone through a balance between vasoconstrictors and vasodilators. The maximum cardiac output is determined by the venous return. In general, prescribing fluids will increase the venous return, increase atrial stretch and stroke volume and, therefore, increase cardiac output. Cardiac output is the product of stroke volume and heart rate, as per the equation below[7]
. Cardiac output is reduced by arrhythmias and a high afterload (i.e. high vascular resistance).
Cardiac output = stroke volume x heart rate
The contractility of the heart (and therefore stroke volume) can be increased with inotropes and the heart rate can be managed with chronotropes. Anti-arrhythmics are negative chronotropes that slow the heart rate until normal rhythmicity, coronary perfusion and ventricular filling return (or at least become sufficiently close so that normal contractility occurs).
Hypovolaemia
Dehydration is the simplest form of hypovolaemia, and occurs when the body loses more fluid than it takes in. Dehydration affects the entire body; for example, there must be sufficient blood volume and kidney perfusion for the kidneys to filter the blood effectively. Kidney perfusion represents a quarter of cardiac output; therefore, if cardiac output falls, so will kidney function. Consequently, the simplest cause of acute kidney injury (AKI), where the kidneys are not adequately perfused, is dehydration and/or inadequate blood pressure.
In order to maintain vital organ perfusion, the body adapts to hypovolaemia by increasing the heart rate and contractility so plasma will flow faster around body and back to the heart. Therefore, a patient with low blood pressure and a high heart rate (tachycardia) is likely to need fluid to fill the increased blood vessel capacity[8]
. In addition, adrenaline might be secreted to shut down perfusion of the body periphery, thus reducing the effective blood capacity and reversing the vasodilatation.
Patients with severe dehydration (see Box 1) may require hospital admission when their fluid requirements are not adequately met by oral intake[9]
. The administration of IV fluids may be needed if the patient has gut stasis or obstruction. Fluid and electrolyte loss may also be significant if there is severe vomiting or prolonged diarrhoea[10]
. Surgery may produce a significant blood loss that requires a combination of fluids, electrolytes and red blood cells.
Box 1: Symptoms of severe dehydration
The main symptom of insufficient fluid intake is thirst.
Others include:
- Not passing very much urine
- Urine is dark and strong smelling;
- Dry or sticky mouth, coated (‘furry’) tongue, cracked lips;
- Feeling dizzy, especially when the patient stands up;
- Reduced skin turgor;
- Low blood pressure;
- Altered level of consciousness.
Sources: National Institute for Health and Care Excellence. Intravenous fluid therapy in adults in hospital. Clinical guideline [CG174][1]
; Tomlin M. Fluid balance. In: A Gray, J Wright, L Bruce & J Oakley. Clinical Pharmacy pocket companion
[8].
Fluid balance
It is too simplistic to consider fluid balance as a patient’s total fluid input minus their fluid output, as this ignores the redistribution of fluid and electrolytes between different body compartments[8]
.
Metabolising nutritients generates energy in the form of ATP, as carbohydrates are broken down into carbon dioxide and water, generating around 300mL of metabolic water each day. Furthermore, patients will drink and IV fluids may be administered. In addition, there is water in food, which contributes towards fluid intake. However, as adequate fluid intake varies with body size, ideal water intake is described as 25–30mL/kg/day (around 1mL/kg/hour)[11]
.
Fluid output
The notional average 70kg person has a urine output of 1.5–2L/day (0.5–1mL/kg/hour). Oliguria is a symptom where a person does not produce enough urine to clear renally excreted body waste (400mL/day or 25mL/hour). Anuria (virtually no urine) or producing less than 10mL/hour is likely to lead to accumulation of toxic metabolites, particularly nitrogenous breakdown products of proteins (e.g. urea, glycine and ammonia) and can cause drowsiness, confusion and delirium.
Insensible losses are water loss that is rarely measured or recorded, including:
- Perspiration from the skin (around 900mL/day), which increases on a hot day, during exercise and if the patient has fever;
- Exhaled moisture from the lungs (around 400mL/day);
- Water lost through faeces (around 200mL/day); however, this is greater in patients with diarrhoea.
It should be noted that vomiting or gastric aspiration may also result in fluid loss.
Surgical drains that are inserted into the body may result in fluid loss, as can surgical wounds (loss by evaporation) unless covered by a dressing. Unseen fistulae (abnormal tubular connections) between body compartments and the exterior (e.g. abdominal to colonic pathways) may also result in fluid loss.
Compounds with a molecular weight >70kDa are too large to pass easily through the pores in the vascular membrane. Therefore, these macromolecules exert a colloid osmotic pressure and hold water in the vasculature. Fluid redistribution occurs where the hydrostatic pressure exceeds the colloid osmotic pressure. Decreasing blood pressure will reduce oedema formation. Giving IV albumin may also decrease oedema by restoring the balance in patients with a high blood pressure. Patients with high blood pressure tend to form tissue oedema and this effective hypovolaemia drives tachycardia. Coronary perfusion decreases during tachycardia, which can cause heart failure. Thus, reducing a high heart rate can improve cardiac performance.
Malnourished patients
Patients who are starved for more than seven days, or malnourished owing to low appetite caused by their illness, will adapt their electrolyte composition. This is because they are deprived of ATP and can no longer maintain the normal electrolyte disposition. Sodium will move into the tissues (serum levels will correspondingly fall) and water will follow, producing plasma hyponatraemia and peripheral oedema (see Figure 2). Potassium will leach out of the tissue into the plasma, but the patient may present with normokalaemia as the excess potassium is passed in the urine. When these patients are artificially fed (enterally or parenterally), they may exhibit refeeding syndrome (the potentially fatal shifts in fluids and electrolytes that may occur in malnourished patients receiving artificial refeeding)[12]
. The rapid increase in plasma glucose activates insulin secretion and glucose moves rapidly into the tissues. Sodium and water will return to the plasma and this may produce stress on the heart. At the same time, potassium, magnesium and phosphate will move into the tissues, predisposing the patient to cardiac arrhythmias. Magnesium and thiamine (vitamin B1) are essential co-factors for the sodium–potassium ATPase pump; therefore, these are often supplemented intravenously if there is high risk of arrhythmias occurring. This is important because giving IV fluids to starved patients is particularly challenging; glucose-containing fluids can cause refeeding syndrome, and so must be managed carefully to avoid cardiac arrhythmias.
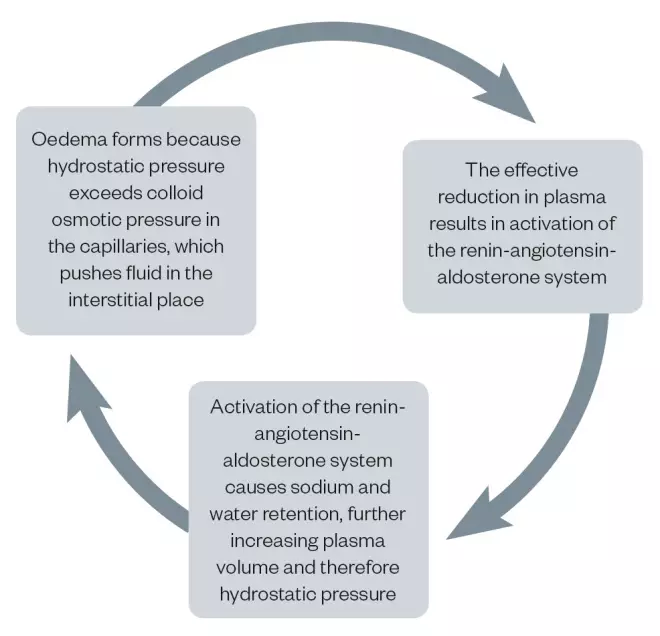
Figure 2: The cycle of oedema formation
Source: MAG/JL
The formation of oedema begins when hydrostatic pressure exceeds oncotic pressure.
Assessing IV fluid needs: ‘the five Rs’
Patients’ fluid and electrolyte needs are assessed through a variety of parameters, including blood pressure and chemistry (i.e. urea, creatinine, potassium, sodium and chloride levels); pulse; capillary refill time and presence of oedema (peripheral and pulmonary)[1]
. Depending on the outcome of the assessment, NICE recommends that IV fluids are prescribed for one of the five Rs:
- Resuscitation;
- Routine maintenance;
- Replacement (of abnormal losses);
- Redistribution (effects);
- Re-assessment.
Resuscitation
Fluid resuscitation is required in situations where a patient is experiencing acute circulatory shock or intravascular volume depletion. The objective is to restore circulating blood volume and increase cardiac output, thereby restoring tissue perfusion and oxygen delivery. Patients who are hypovolaemic have poor venous return to the heart and, therefore, low cardiac output (unless their body has adapted with tachycardia). Increasing blood fluid volume in these patients should improve venous return, increase cardiac output, raise blood pressure and reduce heart rate. NICE recommends a crystalloid solution containing at least 130mmol/L sodium[1]
. An ideal resuscitation fluid is NaCl 0.9% as it contains 154mmol/L sodium. This is sometimes referred to as normal saline (abbreviated N/S); however, this is now seen as an inappropriate descriptor because it has a higher sodium content than plasma (140mmol/L). In addition, the sodium is paired with chloride (154mmol/L) ions; this is significantly higher than plasma chloride (101–111mmol/L). Another suitable resuscitation fluid is Hartmann’s solution (Na+ 131mmol/L), which is also known as ‘compound sodium lactate’ in the UK (see Table 2). In the United States, a similar solution called Ringer’s lactate is used.
Table 2: Electrolyte composition of 1L of common fluids | ||||
| Common fluids | Na+ (mmol/L) | Cl– (mmol/L) | K+ (mmol/L) | Lactate (mmol/L) |
| NaCl (‘normal saline’) 0.9% | 154 | 154 | 0 | 0 |
| Compound sodium lactate (Hartmann’s) | 131 | 111 | 5 | 29 |
| Glucose 4%; saline 0.18% | 31 | 31 | 0 | 0 |
| Potassium 0.3%; glucose 4%; saline 0.18% | 31 | 71 | 40 | 0 |
Cl–: chloride; K+: potassium; Na+: sodium Source: Data taken from the Electronic Medicines Compendium | ||||
Resuscitation is often achieved by a series of fluid challenges (250–500mL crystalloid) administered over 15 minutes until normal blood pressure is achieved. Where there are concerns about the ability of the heart to respond, 250mL is chosen. Blood pressure targets include central venous or jugular venous pressure. Invasive monitoring also produces mean arterial pressure (MAP). Where fluid challenges improve blood pressure, the patient is considered to have been previously hypovolaemic. If the MAP is sustained, resuscitation is complete and consideration can be given to routine maintenance. Targets vary from a well-perfused patient with warm peripheries to those who target an adequate urine output.
Where there are concerns about the ability of the heart to respond to fluid challenges, the passive leg raise can be tried (see Box 2)[1],[13]
. This is seen as a simple, effective, reversible fluid challenge that is non-invasive. However, after 2L of resuscitation fluid and no response, healthcare professionals should seek expert help as the patient’s condition may be a result of sepsis, profound capillary leak (redistribution) or abnormal losses (e.g. internal bleeding).
The timing of fluid replacement and resuscitation can sometimes be as important as the volume and type of fluid administered. Studies investigating the timing of resuscitation for critically ill patients have shown that aggressive and early fluid resuscitation (i.e. patients receive most of their resuscitation fluids within six hours of deterioration, along with other interventions if required) achieves better outcomes than delayed fluid resuscitation (i.e. most fluids are administered more than six hours after the start of deterioration)[14],[15]
.
Box 2: Passive leg raises
This bedside technique can be used to assess fluid responsiveness in a patient, although there are many caveats. It is an easily reversible fluid change that moves blood from the legs to the thorax, effectively increasing venous return and cardiac output.
The patient should initially be semi-recumbent and then their entire bed should be tilted through 45°. Alternatively, it can be performed by lying the patient flat and passively raising their legs to greater than 45°. If, at 30–90 seconds, the patient shows signs of haemodynamic improvement, volume replacement may be required.
If the condition of the patient deteriorates — in particular if they become breathless — the patient may be experiencing fluid overload.
Source: National Institute for Health and Care Excellence. Intravenous fluid therapy in adults in hospital. Clinical guideline [CG174]. Available at: https://www.nice.org.uk/guidance/cg174/ (accessed November 2018)
Routine maintenance
For patients who require maintenance fluids (and who have healthy kidneys and no comorbidities that would affect fluid homeostasis), administering a glucose-based fluid and a second, usually sodium-based, fluid to boost intravascular volume is suitable[16]
. This fluid intake should be sufficient to maintain an even or stable fluid balance. Ideally, it should be given via the normal oral route or via enteral tube feeding. Where these techniques fail, fluid can be administered via an IV cannula[9]
.
The volume dose is 1mL/kg/hour or 25mL/kg/day or 2L for a 70kg patient, and the composition should match that of normal plasma. Patients should be given electrolyte doses of 1mmol/kg/day each of potassium, sodium and chloride (see Table 3).
Table 3: Recommended doses of daily fluid and electrolytes | |||
| Water | Sodium (Na+) | Potassium (K+) | Chloride (Cl–) |
| 1mL/kg/hour | 1mmol/kg/day | 1mmol/kg/day | 1mmol/kg/day |
| Source: National Institute for Health and Care Excellence[1] | |||
Table 4: Electrolyte composition of 1L of common fluids | ||||||||||||
| Diluent 1 | % | Diluent 2 | % | mL | Add | g/mmol | % | Na+ (mmol) | K+ (mmol) | Cl– (mmol) | CHO (g/L) | CHO (kcal/L) |
| NaCl | 0.18 | Glucose | 4 | 1,000 | K+ | 3/40 | 0.3 | 30 | 40 | 70 | 40 | 160 |
| CSL | 1,000 | 131 | 5 | 111 | ||||||||
| 1,000 | 3/40 | 40 | 50 | 200 | ||||||||
| NaCl | 0.9 | Glucose | 5 | 1,000 | K+ | 2/27 | 154 | 27 | 181 | |||
| CHO: carbohydrate; Cl–: chloride; CSL: compound sodium lactate; Na+: sodium; NaCl: sodium chloride; K+: potassium | ||||||||||||
| Mg2+ (mmol/L) | Ca2+ (mmol/L) | PO43- (mmol/L) | Na+ (mmol/L) | K+ (mmol/L) | Cl– (mmol/L) | |||||||
| Plasma | 0.8 | 2.3 | 0.8 | 140 | 4.5 | 106 | ||||||
| Ca2+: calcium; Cl–: chloride; K+: potassium; Mg2+: magnesium; Na+: sodium; PO43–: phosphate Source: Mark Tomlin | ||||||||||||
If no other nutrients are provided, the IV maintenance fluid should contain 400kcal (100g) of glucose to maintain intake and avoid ketosis (from fat metabolism). Table 4 illustrates the composition of common IV fluids. An average volume per day (1mL/kg/hour) of routine maintenance fluid is equivalent to about 2L per day. Target electrolyte requirements are 1mmol/kg of K+, Na+ and Cl–. For a 70kg patient this is 70mmol of K+, Na+ and Cl–. Table 4 therefore shows that for a 70kg patient, 2L per day of glucose 4% and NaCl 0.18% with 40mmol/L potassium would provide an ideal fluid and electrolyte maintenance. Prescribing 2L of saline 0.9% with potassium would provide 300mmol sodium and 360mmol chloride, which would be enough electrolytes for four days.
Redistribution and replacement of abnormal losses
Fluid losses should be replaced by IV bags that contain all the electrolytes that have been lost[1]
. This can only be done by knowing the electrolyte components of these losses and by being familiar with the composition of IV bags. Pharmacists and healthcare professionals should, therefore, know the sodium content of saline 0.9%, Hartmann’s and glucose and saline combinations.
Unusual losses include, but are not limited to, vomiting and nasogastric tube loss, biliary drainage loss, diarrhoea, sweating and pancreatic/jejunal fistula/stoma loss. Each of these losses have different electrolyte compositions[1]
.
Table 5: Electrolyte composition of different fluid outputs | |||||
Sodium (mmol/L) | Potassium (mmol/L) | Chloride (mmol/L) | Hydrogen (mmol/L) | | |
| Vomit | 20–60 | 14 | 140 | 60–80 | 0 |
| Diarrhoea | 30–140 | 30–70 | 0 | 0 | 20–80 |
| Source: National Institute for Health and Care Excellence[1] | |||||
Significant vomiting or diarrhoea can cause large electrolyte losses that must be replaced (see Table 5). While saline 0.9% is an ideal resuscitation fluid, it is probably overused as a maintenance fluid and can cause hyperchloraemic acidosis, reduced kidney perfusion and AKI.
Prescribers should know the patient’s fluid status and plan which IV fluids to provide over the coming 24 hours, rather than prescribing one bag after another. This raises the next most important recommendation from the NICE guidance — review or reassessment.
Assessment or reassessment of fluid status
Regular fluid challenges can be used to assess the patient’s current fluid status. For example, 250mL of saline 0.9% administered over 15 minutes is used to assess the fluid’s impact on blood pressure (central venous or jugular venous pressure). If the patient improves then fades, further resuscitation is needed. If the patient becomes unwell and starts coughing up pink sputum (pulmonary oedema), they are now overloaded and need IV diuretics or they have been tipped into cardiac failure.
The passive leg raise (see Box 2) can also help in assessing patients because it is fundamentally an easily reversible fluid challenge.
Most patients in hospital who have low blood pressure (or a compensatory tachycardia) are considered hypovolaemic until proven otherwise.
Role of the pharmacist
Pharmacists can make a significant contribution by understanding the sodium content of the many drugs and diluents that are required to deliver. Knowledge of formulation and access to the summary of product characteristics (or paediatric formularies) are useful sources for this. Table 6 illustrates some of these factors; however, it should be noted that results may vary by brand.
Table 6: Sodium content of intravenous drugs and diluents | |||||||
| Drug | Form | Strength | Sodium content (mmol) | Daily sodium (mmol) | Diluent | Sodium content (mmol) | Total daily sodium (mmol) |
| Piperacillin and tazobactam | Vial | 4.5g | 11.35 | 34.0 | 100mL saline 0.9% | 15.4 | 80 |
| Erythromycin | Vial | 1g | 0.0 | 0.0 | 1,000mL saline 0.9% | 154.0 | 616 |
| Clarithromycin | Vial | 500mg | 1.0 | 2.0 | 250mL saline 0.9% | 38.5 | 79 |
| Co-trimoxazole (for Pneumocystis carinii pneumonia) 64kg | Vial | 480mg/5mL | 1.7 | 27.2 | 500mL glucose 5% | 0.0 | 27 |
| Pabrinex® (Kyowa Kirin) 1 pair | Vial | 1 pair/5mL | 6.8 | 41.0 | 100mL saline 0.9% | 15.4 | 87 |
Source: Data taken from the Electronic Medicines Compendium Piperacillin and tazobactam 4.5g in 100mL saline 0.9% three times daily = 80mmol/day Erythromycin 1g in 1L saline four times daily = 616mmol/day Clarithromycin 500mg in 250mL saline 0.9% twice daily = 79mmol/day Co-trimoxazole 120mg/kg for 64kg patient implies 16 amps (4 amps in 500mL four times daily) = 27mmol/day Pabrinex 2 pairs in 100mL saline 0.9% three times daily = 87mmol/day | |||||||
Table 6 shows that prescribing Tazocin® (piperacillin and tazobactam; Pfizer, Surrey, UK) 4.5g three times per day in 100mL NaCl 0.9% will add 80mmol sodium to the patient, which is likely to be their total sodium requirement for 24 hours. Erythromycin should be diluted in 1L of fluid for peripheral administration (brand recommendations vary); this adds over 600mmol of Na+. Diluting erythromycin with glucose produces a less stable mixture, but significantly reduces the sodium load. If a central venous catheter is available, 1g can be given in 100mL, thereby reducing the sodium load to 62mmol. Changing the macrolide to clarithromycin reduces the dose frequency to twice per day and the diluent volume to 500mL per day and, therefore, the sodium load to 79mmol. Co-trimoxazole for Pneumocystis jiroveci
or P. carinii (120mg/kg) produces a calculated daily dose of 15–25 amps of 480mg. The daily dose is usually divided up into four portions. It can be very helpful to divide into whole amps and dissolve each dose in 500mL of a given diluent to facilitate administration; however, this is often difficult to prescribe. This huge volume load can be reduced if central venous access is available. Pabrinex® (Kyowa Kirin, Tokyo) dosage can vary, but a high dose in patients with alcohol addiction also delivers a significant sodium load.
Other important formulation questions arise when using effervescent tablets, which often contain sodium bicarbonate (see Table 7). Many newer orodispersible tablets do not contain sodium.
Table 7: Sodium content of soluble/effervescent tablets | ||||
| Product | Dose | Sodium (mmol) | Potassium (mmol) | Phosphate (mmol) |
| Paracetamol soluble | 1g | 19.6 | 0 | 0.0 |
| Sando-K® (HK Pharma) | 1 tablet | 0.1 | 12.0 | 0.0 |
| Phosphate Sandoz® (HK Pharma) | 1 tablet | 20.4 | 3.1 | 16.1 |
| Prednisolone soluble | 5mg tablet | 1.2 | 0.0 | 0.0 |
| Source: Data taken from eMC | ||||
Summary
Achieving optimal hydration is an essential element of holistic patient care. Pharmacists and healthcare professionals need be aware of the five Rs for IV fluid therapy in adults in hospital, and be able to recognise the consequences of mismanaged IV fluid therapy (e.g. pulmonary oedema, peripheral oedema, and volume depletion and shock). Owing to the lack of literature, NICE recommends that further research is needed about the incidence of complications during, and as a result of IV fluid therapy[1]
.
Financial and conflicts of interest disclosure
The author has no relevant affiliations or financial involvement with any organisation or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. No writing assistance was used in the production of this manuscript.
- This article was updated on 18 December 2018 to amend an error in Table 7. Sando-K’s sodium content and Phosphate Sandoz’s phosphate content were each 0.1mmol lower than what is accurate. Both have now been corrected.
References
[1] National Institute for Health and Care Excellence. Intravenous fluid therapy in adults in hospital. Clinical guideline [CG174]. 2017. Available at: https://www.nice.org.uk/guidance/cg174/ (accessed December 2018)
[2] Finfer S, Bellomo R, Boyce N et al.; SAFE investigators. A comparison of albumin and saline for fluid resuscitation in the intensive care unit. N Engl J Med 2004;350(22):2247–2256. doi: 10.1056/NEJMoa040232
[3] Lewis SR, Pritchard MW, Evans DJW et al. Colloids versus crystalloids for fluid resuscitation in critically ill patients. Cochrane Database Syst Rev 2018;8:CD000567. doi: 10.1002/14651858.CD000567.pub7
[4] Bunn F & Trivedi D. Colloid solutions for fluid resuscitation. Cochrane Database Syst Rev 2011;3:CD001319. doi: 10.1002/14651858.CD001319.pub5
[5] Berne RM, Levy MN, Koeppen BM & Stanton BA. 2004. Physiology 5th Ed. Mosby, St Louis MO.
[6] Physicians Now Urgent Care. IV Fluids Services at Physicians Now Urgent Care in Rockville, MD. Available at: https://myphysiciansnow.com/urgent-care-services/iv-fluids/ (accessed December 2018)
[7] Chapter 4: The heart and circulation. In: Green JH. An introduction to Human Physiology (4th edn). Oxford Medical Publications. 1976
[8] Fluid balance. In: A Gray, J Wright, L Bruce & J Oakley. Clinical Pharmacy Pocket Companion 2nd Ed. Published by Pharmaceutical Press. 2016
[9] Huang LH, Anchala KR, Ellsbury DL & George CS. Dehydration treatment and management. 2017. Available at: https://emedicine.medscape.com/article/906999-treatment (accessed December 2018)
[10] Potter L & Wynter S. Intravenous (IV) fluid prescribing in adults. 2017. Available at: https://geekymedics.com/intravenous-iv-fluid-prescribing-adults/ (accessed December 2018)
[11] Sterns RH. Maintenance and replacement fluid therapy in adults. 2017. https://www.uptodate.com/contents/maintenance-and-replacement-fluid-therapy-in-adults (accessed December 2018)
[12] Mehanna HM, Moledina J & Travis J. Refeeding syndrome: what it is, and how to prevent and treat it. BMJ 2008;336(7659):1495–1498. doi: 10.1136/bmj.a301
[13] Monnet X & Teboul J-L. Passive leg raising: five rules, not a drop of fluid! Critical Care 2015;19(1):18. doi: 10.1186/s13054-014-0708-5 (accessed December 2018)
[14] Rivers E, Nguyen B, Hanstad S et al. Early goal-directed therapy in the treatment of severe sepsis and septic shock. N Engl J Med 2001;345:1368–1377. doi: 10.1056/nejmoa010307
[15] Dellinger RP, Levy MM, Carlet JM et al. Surviving sepsis campaign: International guidelines for management of severe sepsis and septic shock. Crit Care Med 2008;36(1):296–327. doi: 10.1097/01.CCM.0000298158.12101.41
[16] Floss K, Borthwick M & Clark C. Intravenous fluids principles of treatment. Clinical Pharmacist 2011;3:274–283. Available at: https://www.pharmaceutical-journal.com/download?ac=1065109 (accessed December 2018)


