


Shutterstock.com
Preventative measures taken across the UK in response to the COVID-19 pandemic have reduced the ability of healthcare professionals to conduct face-to-face clinical consultations. The proportion of GP telephone appointments increased by over 133% in March 2020, as face-to-face GP consultations began to be replaced by either telephone or video consultations[1].
With patients self-isolating, undergoing shielding or simply staying at home, remote consultations offer a way to engage with them while minimising exposure to COVID-19. This makes it an important tool in preventing the spread of the SARS-CoV-2 — the virus causing the disease.
Many pharmacists have experience with consulting remotely by telephone (e.g. when completing a medicines reconciliation or when following up with a patient in community), and techniques to optimise telephone consultations in pharmacy practice have been previously described[2]. Use of technologies supporting remote video consultations is increasing: for example, pharmacies in Wales are piloting the use of consultation software to help return business to usual following the COVID-19 pandemic, and the ‘NHS Near Me’ video service is being trialled in Scotland[3],[4]. With this trend likely to continue, pharmacists will need to adapt and develop skills and strategies to ensure the practice of both video and telephone consultations are effective and person-centred.
As the research literature on remote video consultation is sparse, this article summarises relevant information, advice and best practice principles for pharmacists in relation to remote video consultations[5]. A new ‘CONSULT’ checklist, which recognises the importance of a person-centred approach and shared decision making, is also presented.
Determining the appropriateness of a remote consultation
Remote consultations can be convenient and timely, with reduced need for travel and increased appointment flexibility in timing[6]. Some patients may feel more relaxed at home, but the decision to offer a video consultation may also be used as a method of triage to assess if a face-to-face consultation will be necessary as a follow-up. Moreover, pharmacists should remember that in some cases, especially if you anticipate that a remote consultation for a particular patient may not work, a face-to-face consultation should be attempted from the outset[7].
Figure 1 outlines some examples where video consultations may or may not be appropriate, and outlines an approach that has been adapted for pharmacy from similar resources and tools developed for use in primary care[8], including those by Greenhalgh[9]. Guidance on ethical decision making published by the Royal Pharmaceutical Society may also be helpful in this context[10].
Several challenges, particularly with video consultation, have been reported[11],[12]. For example, the risk of technology failures undermining the confidence of the patient; the increased difficulty of picking up on physical or social cues, including body language; and practical challenges, such as consulting with patients with sight loss, hearing impairment or cognitive impairments, are all important considerations.
Some patients may decline a remote consultation owing to concerns about their personal information being shared using commercial software. Therefore, approved technology and software that does not risk data loss must be used, and pharmacists should be able to reassure the patient of its suitability.
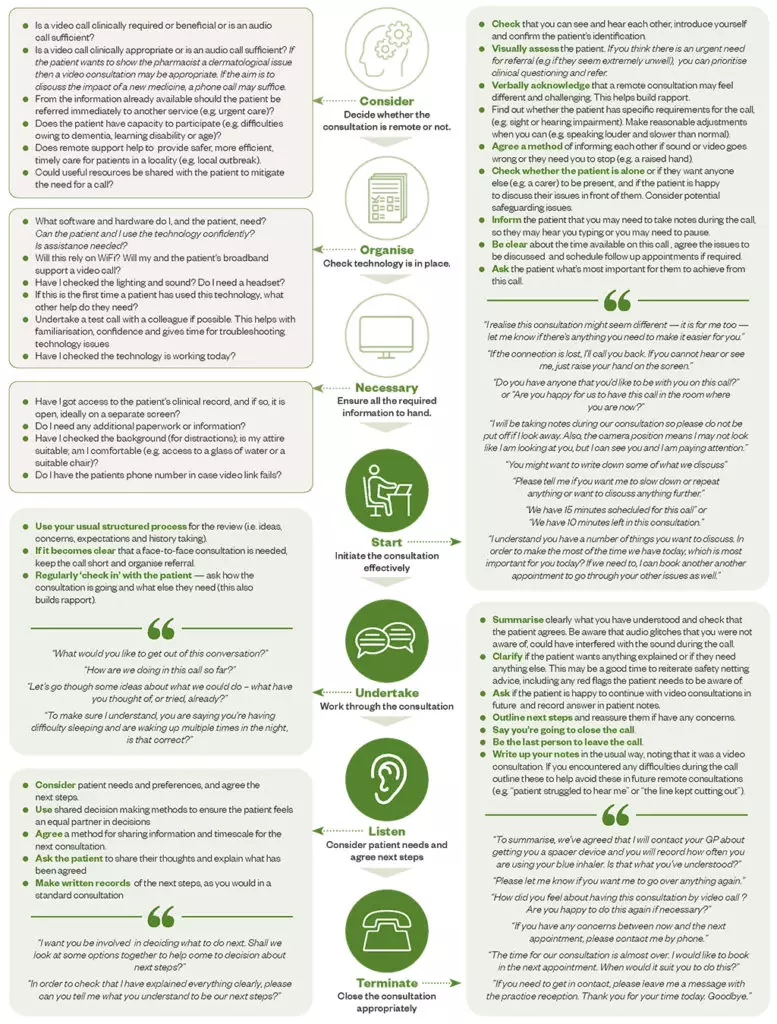
Figure: CONSULT guide to aid pharmacists and pharmacy staff in completing remote consultations
The CONSULT (consider, organise, necessary, start, undertake, listen, terminate) guide can help clarify whether a remote consultation is appropriate and help pharmacists and the pharmacy team understand how to approach the process.
Getting started with remote video consultations
Before the consultation
Remote video consultations require more planning than face-to-face consultations. The acronym ‘CONSULT’ (consider, organise, necessary, start, undertake, listen, terminate) can be used to identify aspects to consider in order to deliver remote video consultations effectively (see Figure, Supplementary Information)[9]. It outlines questions that need to be considered at each stage of the consultation and advice and examples of dialogue that may be helpful.
After considering the appropriateness of a video consultation, pharmacists should ensure that the appropriate technology infrastructure is in place and working, that the environment is suitable and consider how they will undertake the consultation when they cannot examine the patient[13]. Remote consultations should be perceived as equal to face-to-face consultations, with a focus on putting the patient at the centre of their care and understanding their experience.
Checklists and toolkits that aim to support video consultations are also available[14],[15].
Practical considerations
With many pharmacists and patients having little previous experience of consulting remotely by video link, the following practical advice and principles for video consultations should be followed. Much of the advice will also be applicable to telephone conversations.
Technology, equipment and environment
When undertaking remote consultations, the quality and angle of your camera and the lighting in your room can have a significant effect on your interaction with the patient/carer. Consider:
- Positioning the camera level with your eye line, so that you appear to be looking at the patient;
- If you are using two screens, position one above the other rather than side by side, to maintain eye contact with the patient;
- Sitting back and avoid moving forward (e.g. leaning in for emphasis) — this can fill the screen and may not appear natural if the patient is using a mobile phone;
- Confidentiality if using in-built speakers (the pharmacist and patient may want to consider using headphones);
- Sitting with the light towards your face, rather than behind, to ensure the patient can see you;
- The quality of light. If lighting is poor, a ring light can be placed around the camera; daylight (but not bright sunshine) at 90° to the screen is best;
- If you wear glasses, make sure they are clean before you start the call as video cameras can cause strange reflections on dirty glasses. If you have lenses that respond to sunlight, be careful that the room lighting remains constant to prevent them from darkening;
- If working from home, be appropriately dressed and check the background that the patient will see, being aware of personal items, to avoid distractions[16]
.
Interpreting voice and behaviour in a remote consultation
First impressions are vital in a remote consultation. Generally, the level of formality is reduced on video calls, so it is up to you to set and maintain the tone appropriately. Video calls may lead to patients and pharmacists feeling less empowered to discuss issues; therefore, it is important to be proactive in asking what your patient needs to feel comfortable, particularly if they are vulnerable or have a disability. Prior to the call it may be helpful to think about how you will provide reassurance for the patient when discussing sensitive or embarrassing issues remotely (e.g. “I understand that this is not easy to discuss, but I hope the information you provide will help us come up with suitable next steps”).
Interpreting voice intonation, general demeanour and body language is challenging at the best of times, and this difficulty is likely to be amplified in remote consultations. Some non-verbal language is exaggerated by video and some is minimised; for example, sounds such as tuts, ‘umms’, ‘ahhs’ and sighs, that are part of a normal conversation, are often exaggerated and natural gaps in dialogue can seem longer.
Similarly, head movements are intensified in video calls and small eye movements seem exaggerated. There is a need for care when interpreting expressions; some people can look angry, serious or disgruntled when they are concentrating or listening. However, there is a chance that other behaviours will be missed, such as fidgeting or leg shaking.
To mitigate these potential challenges:
- Try to ensure that only one person is talking at a time;
- Keep vocal cues to a minimum — a slow nod or a smile is better;
- Speak slowly and clearly, using clear language and short questions. There may be a need to repeat what is said or to rephrase a question;
- Avoid using filler words (e.g. ‘so’, ‘OK’) as these can dilute the impact of what is being said;
- Show interest and attentiveness by making eye contact and using facial expressions;
- If you need to interrupt the patient, try a visual signal, such as raising your hand;
- Rapid gestures or body movements can be distracting — try to slow them down[16].
Remember that these challenges are intensified for patients whose first language is not English or where there is another communication challenge (e.g. learning disability or aphasia).
Managing emotions
Patients may get emotional on a video call or they may be more demanding about their expectations when not seeing healthcare professionals face-to-face. Be honest that the consultation and way of dealing with problems will be different, but that you will try to help them resolve their issue. If the patient is upset or angry, give them some time and then use silence as needed.
However, to better understand their issue it is important to try to listen, acknowledge and address their concern. Asking the patient about their expectations and what resolution they want is important, but it is then necessary to explain or negotiate what is realistic or possible to achieve during this consultation. The PACE (probe, alert, challenge, escalate) mnemonic can be helpful when consulting with patients who are angry:
- Probe — discover what the issue is, “I can hear you are upset, please let me understand what’s wrong”;
- Alert — try to progress if the patient is shouting, “I need you to stop so we can work this out together”;
- Challenge — state the terms of the consultation, “If you aren’t going to stop shouting, I will have to end this call and we can speak again later”;
- Escalate — following through on your statement, “I am now going to end this call to allow you to pause and we can resume later or reschedule for a later date”[17].
Remember that things may go wrong — as they can with face-to-face consultations — but remaining calm, potentially pausing the consultation and explaining to the patient that you are going to try to resolve the problem can help manage issues as they arise.
Other considerations
If the technology fails during the consultation (e.g. if the audio drops or the patient is accidentally muted) the pharmacist and patient should use the agreed signals (outlined in the CONSULT pathway) that were discussed previously (e.g. a raised hand). In addition, if there is a more general problem with call quality — for example, if audio quality is poor and communication is difficult — then recommending that the patient use headphones or a headset may help.
If the consultation is interrupted by either party, acknowledge it; ask whether the patient wants to wait and complete the consultation or if they would prefer to reschedule. If they wish to continue, wait for them to return and then briefly recap on the last few points you discussed to pick up the conversation.
If there is a need to refer the patient, explain the process and ensure it is appropriate for them (e.g. if they need to speak to their GP, whether they have options to do it remotely). Ask them how they have found the remote consultation and if they found it a barrier to managing their issue; note their answer and preferences on the patient record. If the consultation could have gone better with a third-party present, suggest this to the patient — they may be able to arrange for a relative to be with them for any follow-up consultations[18].
During video calls it may be difficult establishing who should be speaking. This may be caused by delays in the connection. When this happens pharmacists should acknowledge the problem with the patient and either continue or ask the patient to speak. Statements such as “I lost the connection briefly” may help reassure the patient that they have not interrupted you[18]. Pharmacists who are concerned about their skills in delivering a remote consultation (e.g. positioning, lighting) should consider practising with family, friends and colleagues, and asking for feedback to help boost their confidence and improve their technique.
Documentation and post-consultation considerations
In terms of making a record of a remote consultation, this shouldn’t vary from usual practice; the only difference will be to make a record of the medium used, for example, telephone or video. If there is a need for the pharmacy team to follow up with the patient, then this should be recorded in the patient notes and the work calendar if appropriate.
Although not routine in current practice, in some circumstances there may be a desire on behalf of the pharmacist or patient to record the consultation. Although the legalities around this process is outside the remit of this learning article, pharmacists would need to consider the legal requirements within their practice before doing this. For example, the General Medical Council advises doctors that they must inform the patient in advance and obtain consent[19]
.The patient should be told the reasons why the consultation is being recorded, how it will be stored and for how long. It is necessary to record details of patient consent in their records, remembering that the recording will form part of the patient’s record, and should be treated in the same way as other medical or pharmacy records[20].
It is important to remember that remote consultations can feel more draining than face-to-face interaction, especially if the subject matter is emotive. Pharmacists should be diligent in scheduling in breaks and being away from the screen. With this in mind, pharmacists should remember to practise self-care to ensure they can continue to look after their patients.
Useful resources
- Guides for clinicians on remote consultations are available from the
BMJ, University of Oxford and the NHS. - Video consultation information for GPs from the Royal College of General Practitioners and the University of Oxford.
- NHS England has produced a toolkit for online consultations in primary care and the Royal Pharmaceutical Society has produced a podcast on implementing online consultations.
- Barts Health NHS Trust has created a video consultations quick guide for clinicians.
About the authors
Nina Barnett is consultant pharmacist, care of older people, at Northwick Park Hospital, London North West Healthcare NHS Trust & NHS Specialist Pharmacy Service, and visiting professor at Kingston University.
Barry Jubraj is associate director, medicines use and safety team, and visiting senior lecturer at the UCL School of Pharmacy.
Acknowledgements
The authors would like to thank Bernard Richmond QC for his insights into consulting with clients remotely and Zoe Girdis for her helpful comments.
References
[1] NHS Digital. Appointments in general practice — March 2020. 2020. Available at: https://digital.nhs.uk/data-and-information/publications/statistical/appointments-in-general-practice/march-2020 (accessed June 2020)
[2] Sanghera KM. How to do a consultation on the phone. Pharm J 2011;287:249–50
[3] Wickware C. Video consultations to be piloted as part of future plans for community pharmacies. Pharm J 2020;304(7938). doi: 10.1211/PJ.2020.20208032
[4] Burns C. Video consultation system could be offered to all Scottish community pharmacies. Pharm J 2020;304(7937). doi: 10.1211/PJ.2020.20207988
[5] Greenhalgh T, Vijayaraghavan S, Wherton J et al. Virtual online consultations: Advantages and limitations (VOCAL) study. BMJ Open 2016 29;6(1):e009388. doi: 10.1136/bmjopen-2015-009388
[6] NHS England and NHS Improvement. Attending video consultations in secondary care : Patient FAQs. 2020. Available at: https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/04/C0161-video-consultations-patient-faqs-14-april-2020.pdf (accessed June 2020)
[7] NHS England. Millions of patients benefiting from remote consultations as family doctors respond to COVID-19. 2020. Available at: https://www.england.nhs.uk/2020/05/millions-of-patients-benefiting-from-remote-consultations-as-family-doctors-respond-to-covid-19 (accessed June 2020)
[8] General Medical Council. Remote consultations. 2020. Available at: https://www.gmc-uk.org/ethical-guidance/ethical-hub/remote-consultations (accessed June 2020)
[9] University of Oxford. Video consultations: a guide for practice. 2020. Available at: https://bjgplife.com/wp-content/uploads/2020/03/Video-consultations-a-guide-for-practice.pdf (accessed June 2020)
[10] Royal Pharmaceutical Society. RPS guidance on ethical, professional decision making in the COVID-19 Pandemic. 2020. Available at: https://www.rpharms.com/resources/pharmacy-guides/coronavirus-covid-19/coronavirus-information-for-pharmacists/ethical-decision-making (accessed June 2020)
[11] Bakhai M, Croney L, Waller O et al. Using Online Consultations In Primary Care NHS England — implementation toolkit for practices. 2020. Available at: https://www.england.nhs.uk/wp-content/uploads/2020/01/online-consultations-implementation-toolkit-v1.1-updated.pdf (accessed June 2020)
[12] Donaghy E, Atherton H, Hammersley V et al. Acceptability, benefits, and challenges of video consulting: A qualitative study in primary care. Br J Gen Pract 2019;69(686):e586–e594. doi: 10.3399/bjgp19X704141
[13] Wherton J, Shaw S, Papoutsi C et al. Guidance on the introduction and use of video consultations during COVID-19: important lessons from qualitative research. BMJ Lead 2020; In press. doi: 10.1136/leader-2020-000262
[14] NHS Education for Scotland. Video consultation checklist. 2020. Available at: https://learn.nes.nhs.scot/28956/coronavirus-covid-19/remote-consulting-and-recruitment/video-consultation-checklist (accessed June 2020)
[15] NHS England. Using online consultations in primary care: implementation toolkit. 2019. Available at: https://www.england.nhs.uk/publication/using-online-consultations-in-primary-care-implementation-toolkit (accessed June 2020)
[16] Royal College of General Practitioners. Top 10 tips for successful GP video consultations. 2019. Available at: https://www.rcgp.org.uk/about-us/rcgp-blog/top-10-tips-for-successful-gp-video-consultations.aspx (accessed June 2020)
[17] Royal College of Obstetricians & Gynaecologists. Probe, alert, challenge and escalate model. RCOG e-learning website. 2020. Available at: https://elearning.rcog.org.uk/new-human-factors/types-communication/probe-alert-challenge-and-escalate-model (accessed June 2020)
[18] Barts Health NHS Trust. FAQs for clinicians on video consultations. 2020. Available at: https://www.bartshealth.nhs.uk/video-consultations-faqs-for-clinicians (accessed June 2020)
[19] General Medical Council. Making and using visual and audio recordings of patients. 2020. Available from: https://www.gmc-uk.org/ethical-guidance/ethical-guidance-for-doctors/making-and-using-visual-and-audio-recordings-of-patients (accessed June 2020)
[20] GPonline. Conducting online consultations — medico-legal advice. 2019. Available at: https://www.gponline.com/conducting-online-consultations-medico-legal-advice/article/1440537 (accessed June 2020)


