Shutterstock.com / istockphoto.com
Congratulations are due to Pfizer for their reclassification of Viagra (sildenafil) in the UK in November 2017. The move completed a busy year for the Medicines and Healthcare products Regulatory Agency (MHRA) in prescription-only (POM) to pharmacy medicine (P) reclassifications, with two others — an antimalarial tablet and a psoriasis ointment — announced earlier.
The reclassification of Viagra (the PDE5 inhibitor used to treat erectile dysfunction [ED]) is a chance for pharmacists to show how well they can manage its supply. They will have plenty of opportunity to do this; no doubt pharmacies will be mystery-shopped, and the MHRA and important stakeholders will soon judge pharmacy on its results, affecting this reclassification and others.
The UK is not the first to reclassify sildenafil. New Zealand made the move in 2014, and Poland in 2016. But the UK had previously led the way, with pharmacists supplying the medicine under patient group direction for the past 10 years.
The switch to P medicine enables more widespread availability and reduces the burden on GPs. Men will be appropriately informed with an information sheet inside the pack that is tailored to non-prescription availability and communication with pharmacists. If pharmacists in the UK grasp this opportunity, we could see more men being referred for cardiovascular and diabetes checks, or for confirmation and management of a pharmacist’s finding of elevated blood glucose or blood pressure.
Discouraging the use of drugs bought online
The new classification could bring multiple benefits. The first being a decrease in the use of online products for erectile dysfunction — well-stated by the MHRA in its announcement of the reclassification’s approval[1]
. The MHRA has seized £50m worth of unlicensed and counterfeit drugs for ED in the last five years, but plenty more fake goods are likely to have reached their destination. The supply of counterfeit ED drugs is said to be considerably more lucrative than the cocaine trade[2]
.
Sales over the internet typically involve no input from a health professional, and PDE5 inhibitors bought online are likely to be counterfeit, contain more (or less) of the drug than stated, and contain other related compounds and other drugs entirely; for example, hypoglycaemics[3]
.
Anecdotal evidence from New Zealand suggests that some men who have previously purchased ED medicines over the internet are now purchasing from the pharmacist
Alternative remedies for ED can contain unregulated, unlabelled PDE5 inhibitors, their analogues, or other drugs[2]
. In Singapore, 150 people were hospitalised and four people died after they ingested a complementary remedy for ED that was contaminated with a hypoglycaemic and contained an undeclared PDE5 inhibitor. Anecdotal evidence from New Zealand suggests that some men who have previously purchased ED medicines over the internet are now purchasing from the pharmacist without a prescription instead. Following the reclassification in late 2014, fewer packs containing sildenafil were intercepted at the border (Figure 1). The data are not conclusive — a survey on the supply habits of men who use ED drugs could give more insight — but we should be hopeful that reclassifying sildenafil reduces the occurrence of this dangerous practice.
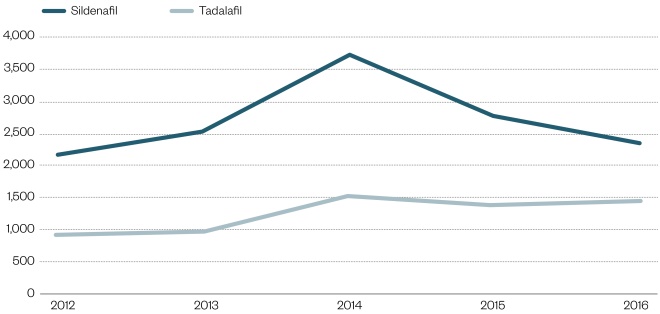
Figure 1: Parcels intercepted by New Zealand Customs Service
Data provided by Medsafe
Note: Drugs known to be counterfeit are excluded.
Creating a safe environment
So how can we encourage men to seek treatment for ED in the pharmacy, rather than online? Keep the embarrassment factor low and make discreet conversation. Educate men on the risks of internet supplies, and certainty of quality from the pharmacy. Make men feel comfortable in requesting repeats; some pharmacists in New Zealand have suggested that men could make eye contact with the pharmacist, or tap on the counter mat, as a signal that they need more ED treatment, rather than asking for the product by name in front of others.
Treating ED earlier
Helping to treat men early in their experience of ED is a second important benefit of reclassifying sildenafil. The condition can negatively affect relationships and quality of life[4]
,[5]
, but many men do not seek treatment because they are embarrassed or do not see the condition as a medical complaint, for example[6]
,[7]
. Again, we need to nurture a comfortable environment in which a pharmacist is readily available for a discreet two-way conversation away from the dispensary. So far in New Zealand, some pharmacists have remarked on having conversations that were easier, more open and rewarding than they expected.
Spotting other conditions during an ED consultation
A third benefit, and one of the most important, is the potential to identify underlying problems before they develop into serious conditions, during consultation in the pharmacy. ED can be a sign of underlying cardiovascular disease, diabetes and myriad other conditions. Pharmacists should consider measuring blood pressure and blood glucose, and refer men who have not had a medical check recently.
Pharmacist refused to supply sildenafil and booked a GP appointment for the patient
Men in New Zealand who request sildenafil from the pharmacist have commonly been referred to the GP for high blood pressure that the man might have been unaware of or ignored, or in cases where the man had not seen a GP for a number of years. Referral can save lives. A man treated by a pharmacist I know returned to the pharmacy to thank her for saving his life. When he requested sildenafil, he had been in denial of his “outrageous” blood pressure and other cardiovascular risk factors. The pharmacist took time to discuss with him her concerns about his cardiovascular risk and his need to take prompt action. She refused to supply sildenafil and booked a GP appointment for him. The man took the necessary steps with his GP to deal with his hypertension and other risk factors, for which he was extremely grateful.
Taking stock of the causes of ED
If pharmacists are to maximise benefits from the reclassification of Viagra, they must consider what might have caused their visitors’ ED — particularly if onset is recent and if it has not been discussed with a GP. Psychological issues may also be important; anxiety, stress or depression can affect erectile function.
Relationship issues should also be considered as an underlying cause. Sildenafil may not be beneficial where relationship problems exist. The man could be advised to open up to his partner about his ED and use of sildenafil.
Limiting the risks of Viagra as a P medicine
Sildenafil’s reclassification comes with risk if it is not handled well. Quick sales should never be made; pharmacists should always have an important conversation with the man that considers the possibility of underlying conditions, contraindications, precautions, and referral where necessary. The pharmacist should remember that the incidence of ED is low in young men, and consider whether the need for the medicine is genuine; while sildenafil is better obtained from the pharmacy than over the internet or from a nightclub dealer, use of the drug as a performance enhancer should be discouraged.
The head of New Zealand’s medicines regulatory agency, Medsafe, sent a clear message to pharmacists following the reclassification of sildenafil in 2014; its use will be monitored and the drug could return to prescription status if the move is not effective. A subsequent audit found areas for improvement, particularly a need for clarification of some aspects of supply. Pharmacy organisations and manufacturers must support pharmacists to supply well.
But pharmacists have the opportunity to improve men’s lives with sildenafil’s reclassification to P medicine; pharmacists must conduct appropriate screenings using the screening tool, consider underlying issues and refer where necessary so that men can continue to obtain treatment for ED through the pharmacy in the future.
Natalie Gauld is a pharmacist and reclassification consultant at Natalie Gauld Ltd. She is an honorary research fellow at the Department of General Practice and Primary Health Care, University of Auckland, New Zealand.
Declarations of interest: Natalie Gauld has received funding for reclassifications including trimethoprim, vaccinations, calcipotriol, adapalene, sildenafil and oral contraceptives. She was on the Medicines Classification Committee in New Zealand (2004–2009). She has acted as a consultant to Green Cross Health, the pharmaceutical industry and pharmacy organisations. She has received travel funding for speaking engagements at conferences from industry and pharmacy organisations. She received unrestricted research grants from Green Cross Health, the Pharmacy Guild, the Pharmaceutical Society of New Zealand and ProPharma for the trimethoprim research. She is a member of the national executive of the Pharmaceutical Society of New Zealand. The opinions expressed in this article are the author’s, and not as a representative of any organisation.
References
[1] Medicines and Healthcare products Regulatory Agency. MHRA reclassified Viagra Connect tablets to a Pharmacy medicine. Available at: www.gov.uk/government/news/mhra-reclassifies-viagra-connect-tablets-to-a-pharmacy-medicine (accessed January 2018)
[2] Chiang J, Yafi FA, Dorsey P et al. The dangers of sexual enhancement supplements and counterfeit drugs to ‘treat’ erectile dysfunction. Transl Androl Urol 2017;6(1):12–19. doi: 10.21037/tau.2016.10.04
[3] Chaubey SK, Sangla KS, Suthaharan EN et al. Severe hypoglycaemia associated with ingesting counterfeit medication. Med J Aust 2010;192(12):716–717. PMID: 2056535
[4] O’Leary MP, Althof SE, Cappelleri JC et al. Self-esteem, confidence and relationship satisfaction of men with erectile dysfunction treated with sildenafil citrate: A multicenter, randomized, parallel group, double-blind, placebo controlled study in the United States. J Urol 2006;175:1058–1062. doi: 10.1016/S0022-5347(05)00418-0
[5] Althof SE. Quality of life and erectile dysfunction. Urology 2002;59:803–810. PMID: 12031357
[6] Nicolosi A, Buvat J, Glasser DB et al. Sexual behavior, sexual dysfunction and related help seeking patterns in middle-aged and elderly Europeans: the global study of sexual attitudes and behaviors. World J Urol 2006;24:423–428. doi: 10.1007/s00345-006-0088-9
[7] Jannini EA, Sternbach N, Limoncin E et al. Health-related characteristics and unmet needs of men with erectile dysfunction: a survey in five european countries. J Sex Med 2014;11:40–50. doi: 10.1111/jsm.12344