

Abstract
Aim
To obtain baseline data for the pharmacy workforce in NHS East of England.
Design
Point prevalence postal/e-mail survey to establish staffing establishments, number of vacancies, number of trainees and qualifications held.
Subjects and setting
Community, academic and industrial pharmacy organisations located in NHS East of England.
Outcome measures
Numbers of pharmacies and pharmacy staff in each sector.
Results
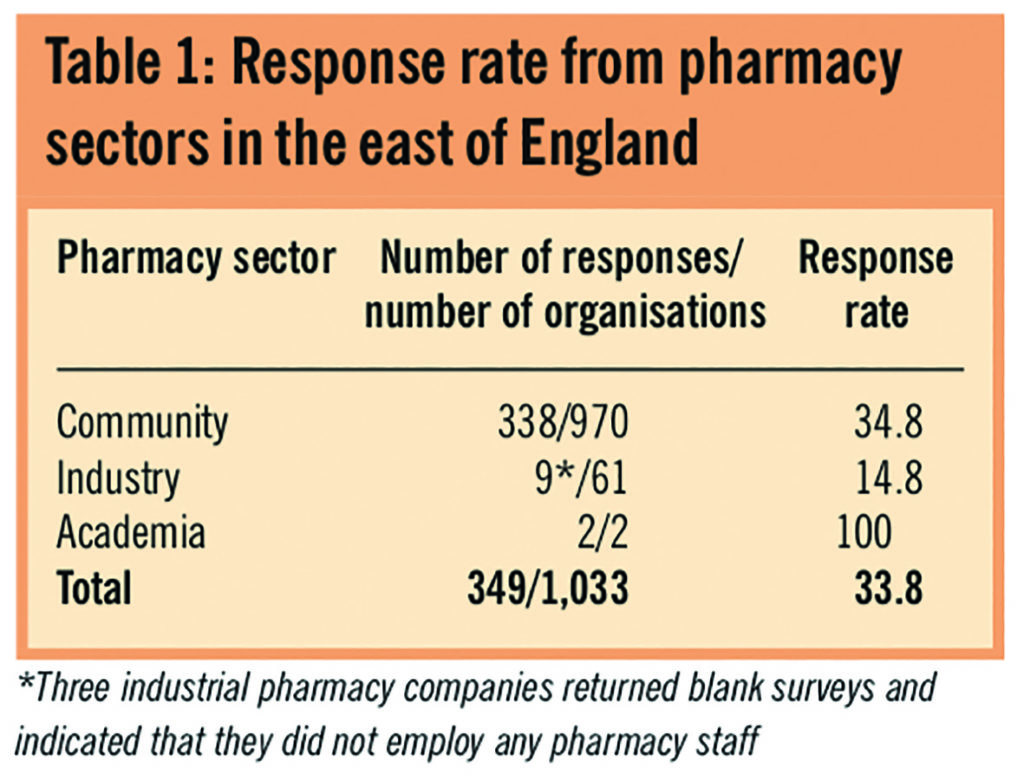
An overall response rate of 33.8% was achieved. Multiple community pharmacies made up the largest group of pharmacy organisations in the geographical area covered by NHS East of England, accounting for 58.7% (n=205). Most pharmacists, pharmacy technicians and pharmacy assistants were working for multiple community pharmacies. The highest proportion of pharmacists and pharmacy technicians were working between 31 and 40 hours per week. The community pharmacist vacancy rate was 36% (293/815 posts), the industrial pharmacist vacancy rate was 15.4% (4/26 posts) and the academic vacancy rate was nil The community pharmacy technician vacancy rate was 34.1% (238/698 posts) and the industrial pharmacy technician vacancy rate was 30.8% (4/13 posts). Of all pharmacist and pharmacy technician vacancies reported most were for posts in the 0–10 hours per week range (81.2% [n=241] and 81.4% [n=197], respectively). Pharmacy organisations accredited to provide training for preregistration trainee pharmacists accounted for 23.6% (n=82) of the total.
Conclusions
This project has obtained current and meaningful baseline workforce data for the community, academic and industrial pharmacy sectors in the East of England. It is important that these data are updated annually and used to inform future pharmacy workforce planning.
Health plays a major role in the economy covered by NHS East of England — Bedfordshire, Cambridgeshire, Essex, Hertfordshire, Norfolk and Suffolk. The population of this region is expanding and becoming increasingly aged. This makes it more reliant on medication, which creates additional demand for healthcare staff. The healthcare workforce in the region faces a number of challenges including a shrinking supply of workers, coupled with stiff competition for potential recruits from other sectors.1
Although data are available from the NHS pharmacy staffing establishment and vacancy survey2 on the pharmacy workforce in the NHS-managed sector in East of England, there is a lack of information on the community, academic and industrial pharmacy workforce and the skill gaps in those sectors. Profiling the workforce by collecting these data is an important first step towards achieving an overall strategy for the pharmacy sector.
Effective workforce planning anticipates potential future imbalances between the supply and demand for different skills in time for action to be taken,3 but it requires information about the pharmacy workforce that goes beyond the census data. To determine the number of staff required to work in all sectors, an understanding of staffing establishments and the number of vacancies is needed.
The future supply of pharmacists and pharmacy technicians cannot be anticipated unless numbers of preregistration placements are known. Skills gaps within the workforce can only be addressed if the qualifications and competencies they possess are identified. An analysis of the training and development needs of the workforce and the infrastructure available to support this is important.
Thus the aim of the project was to obtain meaningful and up-to-date baseline workforce data for the community, industrial and academic pharmacy sectors to complement data collated in the NHS managed sector and inform future pharmacy workforce planning.
Methods
A postal questionnaire was sent to all community and industrial pharmacy premises and e-mailed to the two schools of pharmacy in the NHS East of England area with an explanatory letter in March 2009. The questionnaires were designed specifically for each sector. Those for the community and industrial pharmacy sector covered staffing establishments (including number of hours worked), vacant posts (for pharmacists and pharmacy technicians only), use of locum staff, preregistration trainee pharmacist training and pharmacy support staff training.
The community pharmacy questionnaire asked for information about opening hours, and the academic pharmacy questionnaire asked for data about staffing levels, vacancies and future workforce plans.
The questionnaire was designed to be compatible with form recognition software with tick boxes and minimum free text options. To determine the response rate, each questionnaire was coded according to the premises that it was sent to. Non-responders were followed up via e-mail (if an address was available) and asked to complete the survey during late March/early April 2009.
Community pharmacy contractor addresses were identified from lists held at each primary care trust (PCT). The schools of pharmacy employing academic pharmacists were identified from the list of accredited schools of pharmacy on the Royal Pharmaceutical Society’s website. Industrial pharmacies were identified from the Association of the British Pharmaceutical Industry website and the British National Formulary.4
The data were collated by an external data preparation company. Analysts and data modellers at the NHS workforce review team checked and analysed the data.
Results
Response rate
The response rate to the survey from each sector of the pharmacy workforce is given in Table 1.
Pharmacy organisations are described within PCT boundaries in East of England. The greatest range of pharmacy organisations was found in Hertfordshire PCTs (Table 2). The highest response rate from community pharmacies was from those located in Norfolk PCT (49.1 per cent [n=56] and the lowest from those located in West Essex PCT (19 per cent [n=4]). The distribution of community pharmacies in East of England (based on PCT contractor lists) indicates that Hertfordshire PCTs had the highest concentration (24.7 per cent [n=240]) and West Essex PCT the lowest (2.2 per cent [n=21]). Hertfordshire PCTs’ community pharmacy response rate was 27.9 per cent (n=67). Respondents indicated that most community pharmacies were open 41–50 hours per week (36.1 per cent [n=122]) or 51–60 hours per week (33.1 per cent [n=112]). Only 2.4 per cent (n=8) of all community pharmacies were open for more than 100 hours per week.
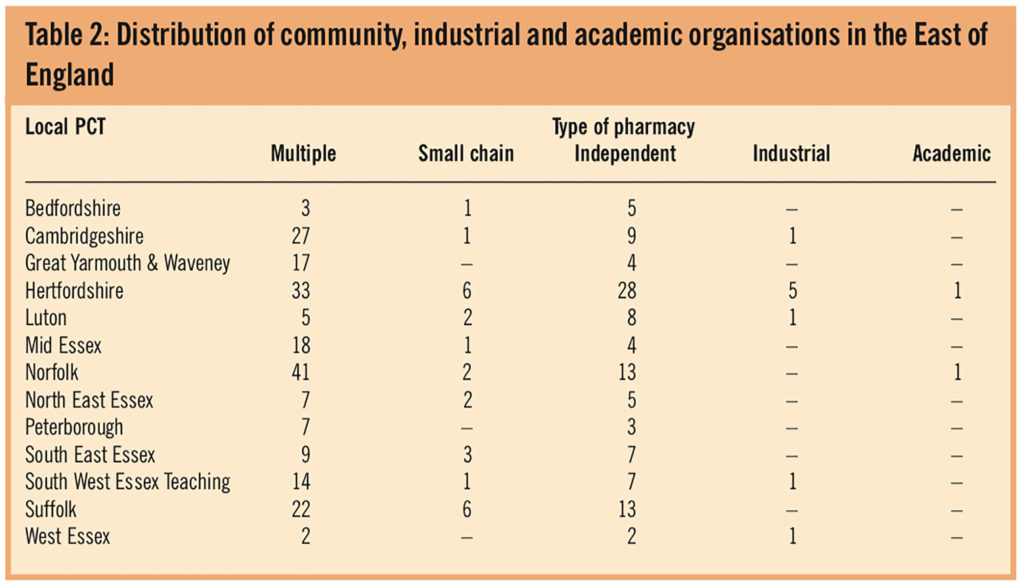
Multiple community pharmacies made up the largest group of pharmacy organisations in East of England accounting for 58.7 per cent (n=205) of all respondents. Independent community pharmacies accounted for 30.9 per cent (n=108); small chain community pharmacies 7.2 per cent (n=25); pharmaceutical industry 2.6 per cent (n=9) and academic pharmacy organisations represented 0.6 per cent (n=2) of the total.
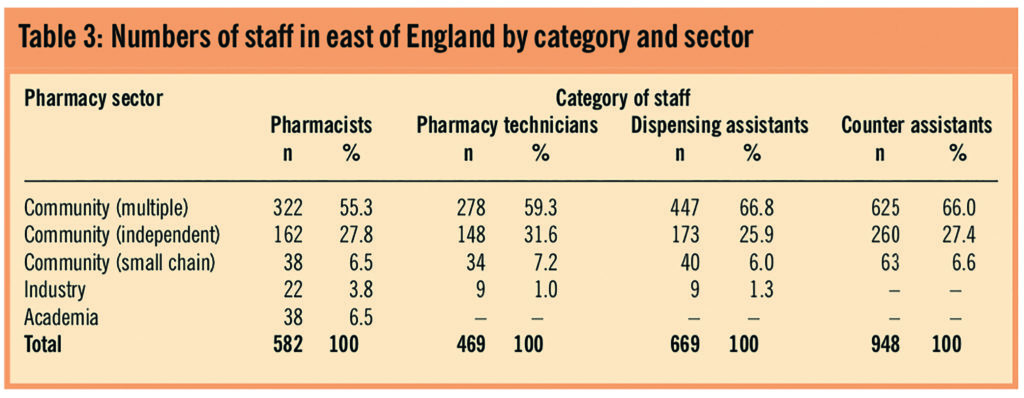
The overall profile of the sector of work for pharmacists, pharmacy technicians, and dispensing and counter assistants in East of England is shown in Table 3.
Pharmacists
Most pharmacists were working either 31–40 or 41–50 hours per week: 33.3 per cent (n=194) of pharmacists were working 31–40 hours and 25.3 per cent (n=147) were working 41–50 hours per week. Some 13.7 per cent (n=80) were working 0–10 hours, 11.5 per cent (n=67) 11–20 hours and 10.5 per cent (n=61) 21–30 hours per week.
The community pharmacist vacancy rate was 36 per cent (293/815 posts), the industrial pharmacist vacancy rate was 15.4 per cent (4/26 posts) and the academic vacancy rate was nil. Of all pharmacist vacancies reported, 81.2 per cent (n=241) were for part-time posts in the range of 0–10 hours per week.
The multiple community pharmacy sector reported the largest number of vacancies at 63.6 per cent (n=189) of the total. The independent community pharmacies reported a vacancy rate of 25.6 per cent (n=76), small chain community pharmacies 9.4 per cent (n=28), and the industrial pharmacies 1.3 per cent (n=4) of all vacancies.
The academic sector reported no pharmacist vacancies (null returns). Most regular locum pharmacists worked at a premises for less than 31 hours a week (73.2 per cent (n=303) worked 0–10 hours per week), were generally recruited from the local workforce and mainly used to cover part-time vacancies. Respondents also stated that they chose to employ a locum rather than sustain a vacancy. An average of 1.2 locum pharmacists were employed by each organisation with an average of 0.9 locum pharmacists used to cover vacant posts.
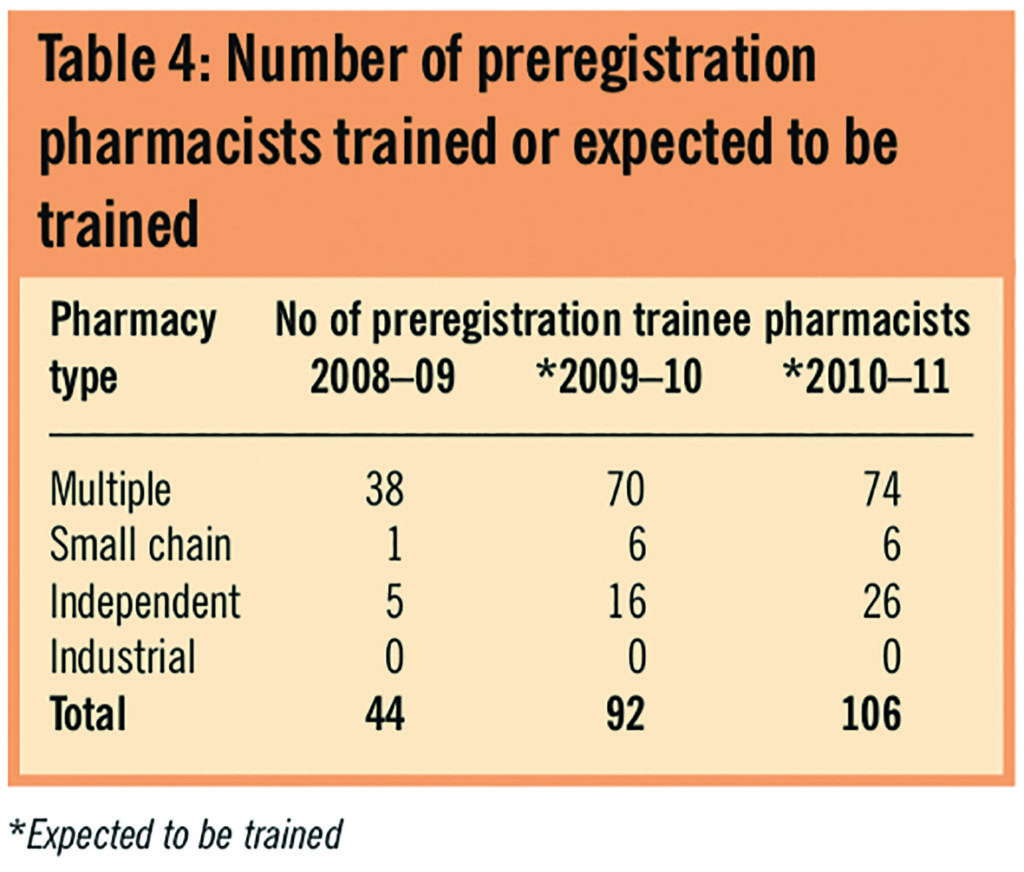
Eighty-two pharmacy organisations (23.6 per cent) were accredited to provide training for preregistration trainee pharmacists (16 per cent [n=87] of pharmacists were also accredited). Table 4 shows the number of preregistration trainee pharmacists who were being trained in 2008–09, and the number of trainees that pharmacy organisations expected to train in 2009–10 and 2010–11. All sectors show an expected increase in the number of preregistration trainee pharmacist training placements.
Pharmacy technicians
Most pharmacy technicians reported working between 31 and 40 hours a week, which accounted for 39 per cent (n=183). Of the remaining respondents 21.7 per cent (n=102) reported working 0–10 hours per week, 21.5 per cent (n=101) 21–30 hours per week, 10.4 per cent (n=49) 11–20 hours per week and 7.2 per cent (n=34) 41–50 hours per week.
The multiple community pharmacy sector represented the largest number of vacancies (64 per cent [n=155]) of all pharmacy technician vacancies reported and the highest number of vacant pharmacy technician posts were part-time positions.
Survey respondents indicated that 59.9 per cent (n=281) of pharmacy technicians held an NVQ level 3 and a technical certificate. Overall, 18.8 per cent (n=88) of all pharmacy technicians reported working as accredited checking technicians.
Pharmacy assistants
Pharmacy assistants were defined in the survey as dispensing or counter assistants. Most dispensing assistants worked 31–40 hours a week (33.6 per cent [n=225] of all pharmacy [dispensing] assistants reported). Most counter assistants worked part time (33.8 per cent [n=320] worked 11–20 hours per week).
The survey reported 33 per cent (n=535) of all pharmacy assistants held an NVQ level 2 Pharmacy Services qualification (or part thereof) across community and industrial pharmacy organisations.
Discussion
Since the data collated were baseline, there are no easy comparators to judge workforce trends. However, where possible the data will be compared to information available from the NHS managed sector or the 2008 Pharmacy Workforce Census.5
Although the overall response rate was relatively low and therefore there are limits to conclusions that can be drawn from these results, the respondents represent a range of different types of pharmacy organisation in PCTs across NHS East of England. A greater response rate may have been achieved if local PCTs or local pharmaceutical committees had distributed the survey rather than the actual distributing organisation (East and South East England Specialist Pharmacy Services). This way the targeted population may not have been aware of the organisation and reasons for distributing the survey.
Since each PCT in East of England provided a list of its community pharmacy contractors, it could be considered to provide an accurate representation of the absolute number of community pharmacy organisations in East of England. Respondents do not necessarily reflect the population as some PCTs were over-represented. A proportion of PCTs displayed low numbers of community pharmacies. Further work will be needed to identify whether this relates to a lack of provision/accessibility or because the needs of the population are being met in other ways or by other providers. Reasons for the multiple community pharmacies being the largest employer of pharmacists, pharmacy technicians and pharmacy assistants could include a greater market share and more competitive salaries.
Since schools of pharmacy are regulated by the Royal Pharmaceutical Society, we can assume that all organisations were identified in this sector. It was more difficult to identify accurately pharmaceutical companies that employ pharmacy staff. The response rate for the industrial sector was extremely low and so it is difficult to draw conclusions. Much of the pharmaceutical industry located in the NHS East of England area was identified in a speculative manner. Indeed, three industrial pharmacy companies returned blank surveys and, when asked why they had done so, indicated that they did not employ pharmacy staff. It may have been helpful to have contacted the Industrial Pharmacists Group to obtain more accurate information and thereby improve the low response rate. However, the Industrial Pharmacists Survey 20086 carried out among the members of the Industrial Pharmacists’ Group, achieved a response rate of 19 per cent — equivalent to the response rate achieved here.
The vast majority of community pharmacies were open to the public up to 60 hours per week — it could be assumed that this range covers traditional shop opening hours of 9am to 5.30pm on weekdays and some weekend opening. The survey did not establish a breakdown of the working day.
Nationally, there has been much debate about 100-hour pharmacies, with increased patient access and improved service provision being cited on the one hand, but the need for more staff that could be utilised in better ways is a contrasting view. There are a number of 100-hour pharmacies in East of England; future surveys could also establish the rate of growth of these premises.
Most pharmacists, pharmacy technicians and pharmacy (dispensing) assistants were working 31–40 hours per week. This compares to latest census data reporting that pharmacists work an average of 35 contracted hours per week.5 A significant percentage of pharmacists who responded to the survey were working over 40 hours per week. Therefore reported actual working hours in East of England could be higher than the national average and could reflect a shortage in supply of pharmacy staff or a policy of not employing additional pharmacists.
Unlike pharmacists, pharmacy technicians and dispensing assistants, most pharmacy counter assistants were working 11–20 hours per week (as well as working across a range of pharmacy hours) and this implies that the make-up of this part of the workforce is different from the others already described.
The fact that a wide range of hours were worked each week across the pharmacy workforce and that most vacancies were part-time supports national evidence that there are large numbers of part-time workers,5 but some of these part-time workers may have other jobs — effectively operating as portfolio workers. The survey did not identify whether members of the workforce held more than one post.
It is interesting to note that not all locum pharmacists were used to cover vacant posts. The average number of employed locums per organisation was higher than the average number of vacant posts. This may provide evidence that locum pharmacists were used to cover permanent staff undertaking other activities. Organisations were generally employing regular locums rather than sustaining a vacancy. This may indicate that the demand for pharmacy services was high.
The results suggest that generally (with one exception) most pharmacy organisations within PCTs did not need to resort to using national agencies (rather than hiring local people) to hire locum pharmacists. Anecdotal evidence before the distribution of the survey had suggested that some locum pharmacists were travelling long distances to premises in East of England.
Not all pharmacies or pharmacists were accredited to support preregistration trainee pharmacist placements so there may be capacity to increase the number of trainees and therefore the supply of pharmacists in the region (assuming that the trainees stay in the region after qualifying). The planned increase in the number of preregistration trainee pharmacist placements over the next two years may be an attempt to reduce current vacancy rates as organisations are trying to grow their own staff.
Future mandatory registration of pharmacy technicians means that minimum levels of qualifications will need to be achieved including an NVQ Level 3 and a technical certificate. Results from the survey indicate that a sizeable number of pharmacy technicians in East of England meet this requirement, however a significant number will need “grandparenting” when mandatory registration becomes law in 2011.
Accredited pharmacy technicians have been final checking dispensed items of prescriptions clinically screened by pharmacists, thereby freeing a large amount of pharmacists’ time to undertake more clinical activities. Community pharmacists are being asked to deliver more clinical services but prescription numbers are rising, so using accredited checking pharmacy technicians could free pharmacists’ time. It will be important for organisations to establish the number of accredited checking pharmacy technicians to achieve acceptable levels of skill mix and productivity.
The Royal Pharmaceutical Society has, since 2005, made it a professional requirement that pharmacy assistants achieve a minimum NVQ Level 2 qualification. Results from the survey indicate that a considerable number of pharmacy assistants still need to achieve this qualification (or part thereof) in the area of pharmacy in which they work. It is not clear how this will be supported.
Ascertaining the full impact of differences between supply and demand for pharmacy staff in East of England is difficult. The survey’s main focus was to establish numbers of staff and vacancies. It is difficult to assess accurately the current demand placed on the pharmacy workforce.
The increasing proportion of elderly people in East of England (who are likely to be more reliant on medication) will increase demand for community pharmacy services. The changing working environment — extended opening hours, legal and regulatory changes (including the responsible pharmacist legislation) — is also contributing to an increase in demand7 so there may be a need for more pharmacy staff or a greater use of skill mix. However, the current economic climate may make further expansion of community pharmacies in East of England unlikely. Most community pharmacies rely on their prescription dispensing business to remain financially viable.
It is likely that the future demand for academic pharmacists will rise because of the need to restructure the core undergraduate curriculum so that it provides meaningful clinical experience (as specified in the pharmacy White Paper8). A review of the preregistration year and whether it sits inside or outside the degree programme will have an impact. The number of schools of pharmacy has been growing nationally and their continued growth could create a potential surge in demand for placements, especially as teaching methods are likely to become more practice-focused.7 East of England may be adequately served with regard to schools of pharmacy, but it is not known how many pharmacy graduates are staying in the region and therefore supplying the pool of pharmacists available to meet demand.
Increased demand for pharmacists from the industrial pharmacy sector is likely to come from a combination of the development of direct patient care specialist services and from the new medicines that will be developed in the coming years.7 Nationally, it has been reported that the supply of traditional industrial pharmacists will probably not rise to meet expanding demands because of the comprehensive changes in skill mix and the increasing use of a wider range of science graduates that have taken place over the past 20 years.7
The high numbers of vacancies described by this survey may provide evidence that there needs to be growth of the pharmacy workforce in the community and industrial sectors in East of England. However, the low response rate suggests that the vacancy rate should be viewed cautiously and further work is needed to establish whether the vacancies described by respondents in this survey translate to the whole pharmacy population in East of England.
A greater sample size used in conjunction with vacancy rates described in the NHS managed sector2 will indicate whether there is also a need to increase the supply of pharmacy staff across the whole of the pharmacy workforce in East of England to meet demand. Encouraging staff to migrate across pharmacy sectors may not solve the problem because the vacancies seem to span all sectors.
Some researchers suggest that certain developments in the profession are likely to have a negative impact on pharmacists’ willingness to stay in community pharmacy. These include the growth of multiples and decline of independent pharmacies, along with a relaxation of control-of-entry regulations for large supermarkets and the development of alternative distribution mechanisms for medicines.9 Future surveys could investigate these trends in East of England.
The survey did not take account of other workforce factors such as age, gender and ethnicity. The impact of e-pharmacy businesses and the introduction of new technology (to increase the efficiency of the prescription dispensing business) were also not included. These factors will all have an impact on services delivered in the future and the number of pharmacy staff employed.
Conclusions
This project has obtained current and meaningful baseline workforce data for the community, industrial and academic pharmacy sectors in NHS East of England. It is important that efforts are made to improve the response rate, that the data are updated annually and used to inform future pharmacy workforce planning.
Acknowledgements
The project was overseen by the East of England Pharmacy Workforce Development Group and delivered by the collaboration of London Pharmacy Education and Training (part of East and South East England Specialist Pharmacy Services), the NHS Workforce Review Team and Skills for Health. I thank Jennifer Fenelon, former East of England regional director for Skills for Health (which funded the project), Tom Skidmore, former senior information analyst with the NHS workforce review team and Jack Turner, information analyst with the NHS workforce review team.
About the author
Christopher John, MSc, MRPharmS is assistant director at London Pharmacy Education and Training and pharmacy adviser to the NHS Workforce Review Team.
Correspondence to: Christopher John, London Pharmacy Education and Training, 50 Eastbourne Terrace, London W2 6LG
e-mail christopher.john@chelwest.nhs.uk
References
- East of England Sector Skills Agreement. Skills for Health. October 2007
- National NHS Pharmacy Staffing Establishment and Vacancy Survey 2008. NHS Pharmacy Education and Development Committee. Available at www.nhspedc.nhs.uk.
- Mullins L, Management and organisational behaviour. London: Pitman Publishing. 1996
- British National Formulary. London; BMJ Group and Pharmaceutical Press, September 2008.
- Hassell K, Seston, L, Eden M. Pharmacy Census 2008: Main findings. London: The Royal Pharmaceutical Society, 2009.
- Al-Ghita F, Halliday J. Industrial pharmacists survey 2008. Pharmaceutical Journal 2008;281:670–1.
- Guest D, Budjanovcanin A, Oakley P. Planning the pharmacy workforce: is there a shortage of pharmacists? Pharmaceutical Journal 2008;281:696–8.
- Pharmacy in England. Building on strengths – delivering the future. London: Department of Health, 2008.
- Guest D, Budjanovcanin A, Oakley P. Planning the pharmacy workforce: will pharmacists stay in pharmacy? Pharmaceutical Journal 2008;281:672–4.


