

Abstract
Aim
To evaluate a new type of automated dispensing system (Consis), in a hospital pharmacy.
Design
Before-and-after study.
Setting
A hospital pharmacy dispensary.
Outcome Measures
Impact of automation on storage space for medicines; dispensing errors; overall efficiency of the department, including staff time.
Results
4.1m2 less floor space (2m3 less total space occupied) was required to store medicines after the introduction of the automated dispensing machine. There was a 16% reduction in dispensing errors identified at the final checking stage. 2.6WTE (19%) fewer staff were needed in the dispensing and restocking process, despite a 19% increase in workload. The quality of the service also improved with faster turnaround of prescriptions.
Conclusions
The Consis automated dispensing system has significantly improved the delivery of a pharmaceutical service to a large acute hospital. The study confirms the findings of an earlier study using a different type of automated system. In view of the size of the system, these results are potentially applicable to both hospital and community pharmacy.
Automation of dispensing in pharmacy has been around for many years. Even back in the 1990s, those of us who attended the mid-year meetings of the American Society of Health-System Pharmacists will have marvelled at the technology available to dispense medicines. The problem was that these machines were designed for unit dose dispensing which is the norm in the US. The other difficulty we had then was that we were working in a mixed dispensing environment with part dispensing from bulk packs and part original packs. This problem was reduced significantly when most manufacturers produced original packs. There are now several different automated dispensing systems available in the UK, all of which are designed to store and pick original packs of medicines.
The main drivers for automating dispensing have been to reduce dispensing errors and increase efficiency, but the use of automation really began to increase when it was recommended in the Audit Commission report “A spoonful of sugar”.1 This gave practical examples of how hospital pharmacy could re-engineer services as advocated by the Department of Health in “Pharmacy in the future”.2 However, there is little published evidence demonstrating the benefits of automation in practice. One of the early implementers of automation has demonstrated that introducing automation does free staff time and reduce dispensing errors.3 More recently, early results from an evaluation of automated dispensing in Wales has suggested similar results.4,5
However, despite a large number of articles written about automation these are the only pieces of hard evidence to emerge from the UK supporting the hypothesis of reduced dispensing errors and increased efficiency. Furthermore, these evaluations have been of one particular type of automated dispensing system.
The various systems available in the UK fall into two distinct types: random storage machines (where the picking head puts the stock to a location determined by the system computer) and the channel storage system (where stock is loaded manually into predetermined channels). The latter can achieve a higher pack storage density than the former.6
The pharmacy at the Royal Wolverhampton Hospitals NHS Trust (RWHT) was the first UK site to have a channel storage-based automated dispensing machine, the Consis system from Baxter.7 The perceived benefits of introducing automation are improved efficiency, enhanced safety and improved use of space.8 Therefore, an evaluation of this system was undertaken to see if these perceived benefits were indeed proven in a different type of automated dispensing machine.
Method
Various parameters related to the dispensing process (space, dispensing errors and efficiency) were evaluated before and after the installation of the Consis system and the area under study acted as its own control.
Results
Space
One of the main drivers for choosing the Consis system over other systems was the fact that it was possible to store more items per square metre. Therefore, before the installation of the machine, the footprint of the existing storage systems was measured. Before the installation of the Consis system, medicines were stored on open shelving on two walls of the dispensary, four Sintek drawer units, and two refrigerators. The total footprint of this mixed storage system was 14.3m2, and occupied a total of 9m3 of space in the dispensary. Medicines were also stored in the Controlled Drugs room but, since CDs were not put into the automated system, the footprint of this area was not included. Following the implementation of automation, medicines were stored in two Consis modules, two Sintek drawer units, and two refrigerators, with no shelving on the walls. Two Sintek drawer units remained in the dispensary to store part packs of medicines returned from wards. After automation, the total footprint of the storage systems in the dispensary was reduced to 10.2m2, ie, 4.1m2 less floor space was required to store medicines. The total space occupied by the storage systems was reduced by 22 per cent from 9m3 to 7m3. This increased availability of floor space proved invaluable as the dispensary was only 77.2m2 in area.
Dispensing errors
Like most hospital pharmacies, we use various grades of staff for dispensing, but within a “safe systems of work” framework. The dispensing process before and after automation is shown in Figure 1.
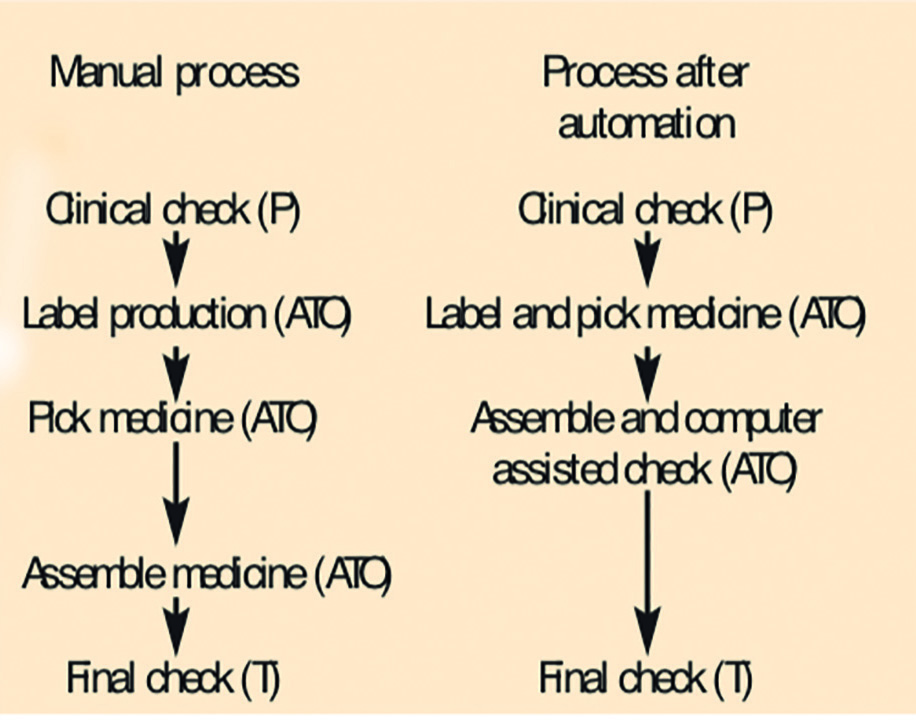
As can be seen from the diagram the department had already modernised its system, with pharmacists only involved in professional/clinical checking before dispensing, and preferably in the ward environment. Since prescriptions were dispensed primarily by assistant technical officers (ATOs), there was always a final check by an accredited pharmacy technician. The impact of automation was to amalgamate the labelling and picking process. Unique to the Consis system is an accuracy check, where the dispensed product is scanned with a bar code reader which compares the actual product dispensed with that ordered when the label is generated. We chose to include this as part of the assembly process (Figure 1) although it could be used to assist the final check by the technician.
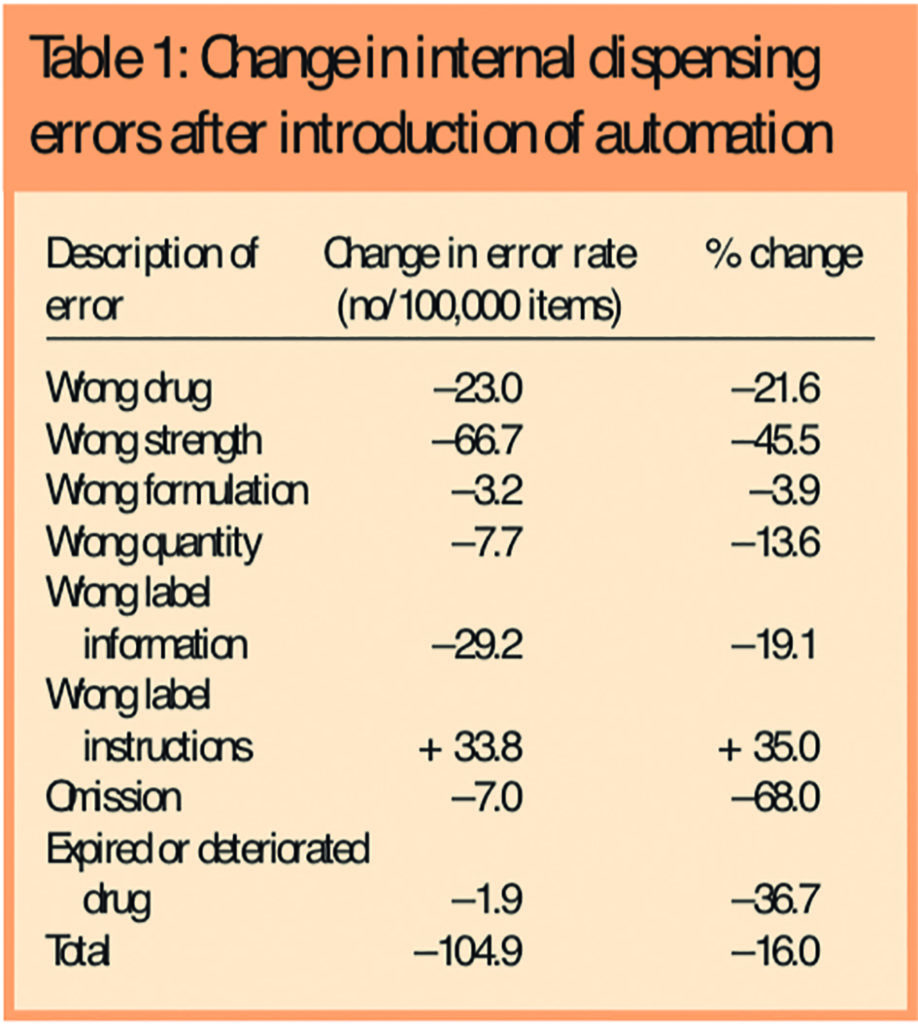
As part of normal performance management within the department logs are kept of all dispensing errors picked up by the technician at the final accuracy checking stage, before the dispensed item is released to the wards. These logs were reviewed for five months before the introduction of the automated dispensing system, and four months after. In the post-automation phase the error log picked up errors from Consis-dispensed items and those still dispensed manually, but did not discriminate between them. The error rate (errors/100,000 items dispensed) in each period was then calculated, and shown in Table 1. As well as the total error rate, Table 1 shows the change in error rate for various aspects of the dispensing process. There was a significant reduction in the overall error rate after the introduction of automation and all categories of error were reduced, with the exception of incorrect label instructions, which increased.
Efficiency
Efficiency of the department was studied by measuring the amount of staff time involved in the dispensing process and restocking.Although the latter is not part of the dispensing process as shown in Figure 1, it is an essential support function. We thought it important to include this in the evaluation, since the Consis machine is loaded manually. Therefore, for a two-week period immediately before the introduction of automation (late August 2003), staff were logged when they were involved in labelling, dispensing, checking or restocking of medicines. As part of the log, a record was kept when staff had breaks or were assigned to other areas of work which did not involve them in the dispensing process. In this way we expected that an accurate picture of staff time involved in dispensing process could be built, rather than just how many staff were in the dispensary. The same exercise was repeated in May 2004 after the Consis system had been in operation for approximately six months. This period was used because the work profile was likely to be similar, since both periods covered the two weeks running up to a bank holiday.
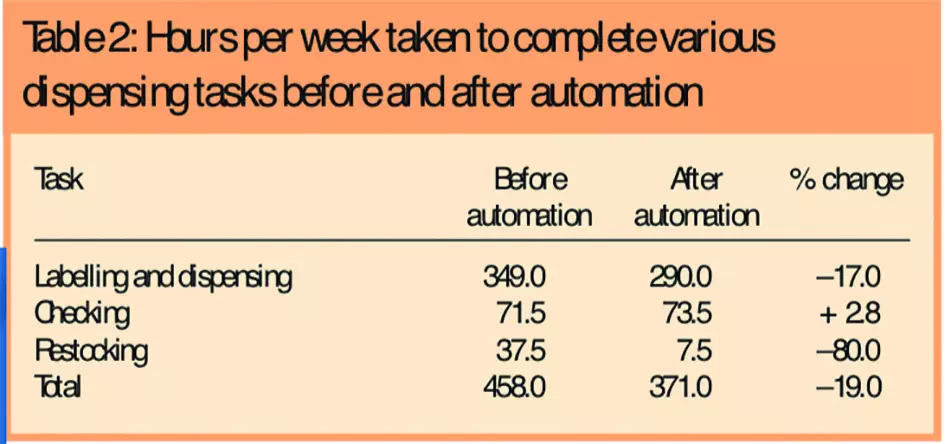
The results (Table 2) show the staff time in three areas of dispensing and labelling (ATO time), final checking (technician time), and re-stocking shelves/Consis machine (ATO time). Not surprisingly the staff time involved in the dispensing of medicines was reduced significantly, but the final checking of prescriptions by an accredited checking technician remained unchanged. Although loading the Consis machine is carried out manually, the results show that the total time required for restocking is much less than restocking conventional shelving.
In addition dispensing data for the two study periods in question were also collated to compare workload, to ensure that staff time figures were not as a result of a reduction in workload. Table 3 shows that the number of items dispensed after implementation of Consis increased by 19 per cent, whereas the total staff time involved in the dispensing processes (from Table 2) decreased by 19 per cent. Table 3 relates only to weekday activity because the staff time activity log was only carried out during the week. Therefore, the actual total dispensing activity for the department is greater than reported here.
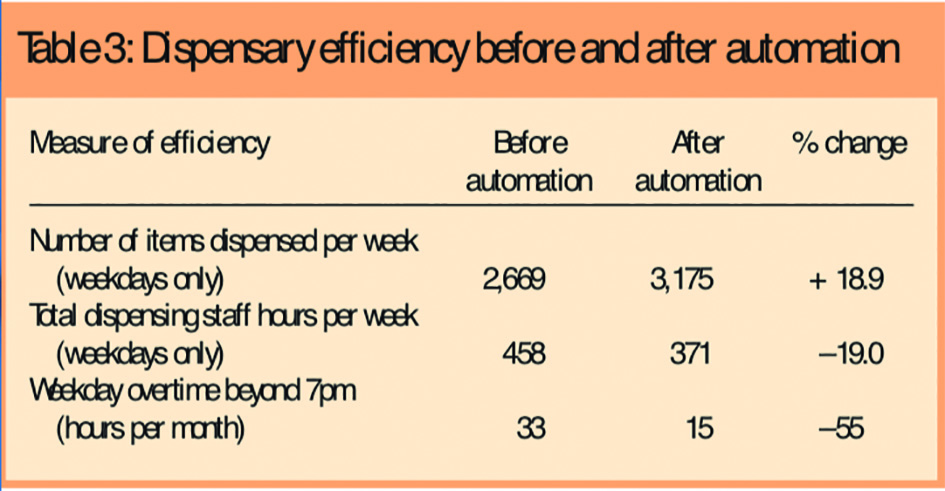
The department operates an extended service in the evenings and, although prescriptions are received until 6pm, staff work until 7pm on a rota basis to clear the work. If the work is not cleared then staff work beyond 7pm and are paid overtime. Therefore, as an indicator of efficiency, the weekday overtime for dispensary staff working beyond 7pm was reviewed for two months before the introduction of Consis and two months after. Table 3 indicates a 55 per cent reduction in weekday overtime worked beyond 7pm following the introduction of Consis.
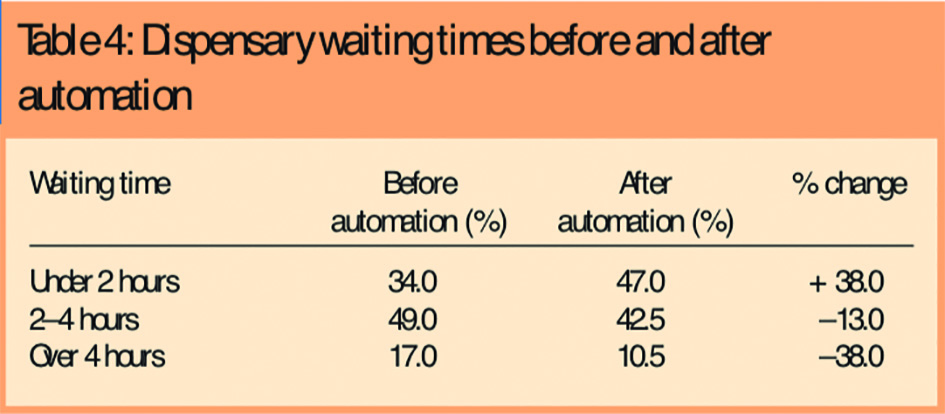
In addition to doing more work with fewer staff, the performance of the department in terms of waiting time also improved. The overall turnaround time for all items dispensed by the inpatient section of the dispensary, was reviewed. Data were taken from our prescription tracking system, which logs a prescription at each stage of its journey through the dispensary from the initial clinical check to the final check. Data were analysed before and after the introduction of automation. Table 4 shows an increase in the number of items dispensed in under two hours, which represents almost half of all items dispensed, with a reduction in the number of items taking more than two hours.
Discussion
The implementation of the Consis automated dispensing system went smoothly, and required minimal enabling works. This is probably due to the simplicity and size of the machine. It is the most space efficient of all the automated dispensing machines in use in the UK holding 3,300 items/m2, which is twice that of the random storage machines.6 This space efficiency is clearly demonstrated by the fact that over 4m2 of floor space was released in our pharmacy as a result of implementing the system. This was particularly important to us as space is at a premium in the department. The dispensary is in a basement and has a confined feel to it. Therefore, the extra floor space helped make the whole dispensary feel less cramped. Furthermore, the actual space occupied by the storage systems was 2m3 less following the introduction of the automated system, which enhanced the working environment.
One of the drivers for introducing automation into the dispensing process is potential reduction in dispensing errors. However, most hospital pharmacies in the UK operate safe systems of work with internal checking of all prescriptions before releasing them to patients. We evaluated the effect that automation had on the internal errors picked up during the final checking process, since this is where the new technology is likely to impact. This element of the study was undertaken by an independent external reviewer, who was only available for a limited time, which is why only four months were reviewed post automation. As can be seen from Table 1 there was an overall reduction in internal errors picked up at the checking stage of 104 per 100,000 items dispensed. Although this is smaller in percentage terms (16 per cent) than reported by Slee et al3 (50 per cent), it is greater in absolute numbers than the initial reports from the Welsh evaluation (equivalent to 30 per 100,000),4 (10–40 per 100,000).5 However, it is difficult to make clear comparisons with these papers since it is not clear whether they refer to internal dispensing errors, as described in this paper, or dispensing errors which have been identified outside the pharmacy. It is interesting to note from Table 1 that the greater reduction in errors was in the picking of the wrong drug or strength, compared with labelling errors. This was expected, as the automated dispensing machine only picks what the operator tells it to, the operator can still generate incorrect information on the label, as the machine does not influence the production of a label.
Improved efficiency has been a key reason to automate the dispensing process, since most hospitals are under pressure to decrease patient waiting times and increase throughput. In this study it was found that, as a result of introducing automation, there was a 19 per cent reduction in staff time (Table 2) involved in the dispensing process and restocking. The total ATO time saved in person hours was 89 hours/week (Table 3) which is the equivalent of 2.4 WTE, and represents 19 per cent of staff working in the dispensary. This is similar to the findings in the first evaluation of automated dispensing in the UK,3 but less in percentage terms than was found in the Welsh study (30–35 per cent).5 It is worth noting that there was no change in technician time involved in checking prescriptions in our study (Table 2), which was expected, since it is the picking part of the dispensing process which has been automated. If this time is excluded from the analysis the actual percentage reduction of staff time increases to 23 per cent. Furthermore, we analysed the time staff were involved in loading the Consis machine, as this was a manual process, but guided by the system software. This element showed a significant reduction in staff time (Table 2), which is in contrast to the first published evaluation of automation in the UK,3 which reported that loading the robot took longer than expected.
Part of the ATO time released has been used to undertake quality improvements such as releasing staff to undertake NVQ2 training, rolling stock checks in the dispensary, and improving other working processes. ATOs have also adopted some more of the technical roles as skill mix has been further reviewed.
It can be seen from Table 3 that not only are fewer staff needed, but more work is being carried out. The driver for this is two-fold.
First, the hospital has increased its activity and, secondly, the pharmacy has introduced a ward-based technician service with “one stop” dispensing. Rather than reduce the number of dispensed items, it has contributed to an increase, since there are fewer stock items used on wards and more individually dispensed items. Furthermore, this additional work comes to pharmacy during the week rather than at weekends, because it is managed by ward-based technicians.
As a result of this improved efficiency some of the ATO time released has been converted into additional technician time to undertake the final check on dispensed items. Not surprisingly the study showed that the number of staff hours involved in this part of the work process did not change following the introduction of automation. However, as the total number of prescriptions dispensed has increased, we thought that, having automated the dispensing process, the checking stage may be the rate-limiting step in the overall system. Furthermore, additional technician time has allowed the dispensary to release staff to support the ward-based technician service, which is a further tangible benefit which staff can see as a result of introducing automation.
The reduction in staff time and increased work done in the dispensary was not at the expense of quality of the service. As discussed previously, the internal error rate was reduced. Furthermore, the overall turnaround time in the dispensary improved as shown in Table 4, with almost half of all prescriptions being completed within two hours. It is expected that this will further improve with the additional checking technicians released from the staffing resource by automation.
In this study we decided to evaluate the turnaround time for all prescriptions, not just discharge prescriptions. This approach was used since the “one stop” dispensing service was introduced over the past year, which should have made an impact on discharge prescriptions. The data presented here should not have been affected by this change in service provision because it relates to all dispensed items and only measures turnaround time in the dispensary. The major impact of the “one stop” dispensing system will be through items being ready labelled for discharge on the wards rather than those coming down to pharmacy for dispensing.
Conclusion
The results presented here confirm those found in the only other published evaluation of automation in the UK3 and are similar to those emerging from work currently being undertaken in Wales.4,5 However, this study evaluates a different type of automated dispensing machine. Thus, it would appear that the benefits of automation are not system-specific.
This study evaluated in detail the three key benefits of automation: improved use of space, reduced dispensing errors, and improved efficiency. We found that the expected benefits8 were in fact realised in practice. Furthermore, this study investigated in detail the impact of automation on the different types of dispensing error, and has demonstrated that the greatest impact was, as expected, on those errors associated with picking the medicine.
Introducing automation requires significant resources but, as the results here have shown, it will result in improved efficiency. The resources released could be used to pay for the investment, or provide extended pharmacy services. These benefits together with the faster turnaround of prescriptions and reduction in dispensing errors make powerful arguments for funding.
Moving this agenda forward in hospitals is important, since introducing automation is part of the Department of Health Medicines Management Performance Framework,9 and is promoted in the NHS “Vision for pharmacy” document,10 which is an update on the original “Pharmacy in the future” document.2
Although this study has evaluated the system in a hospital pharmacy environment, the compact nature of the Consis system, also lends itself well to community pharmacy, and the benefits described here are potentially equally applicable to this environment.
About the authors
Raymond Fitzpatrick, PhD, MRPharmS, is clinical director of pharmacy and professor of pharmacy, Peter Cooke BSc, MRPharmS, is deputy director of pharmacy, Carol Southall is chief technician patient services, Kelly Kauldhar is senior technician patient services and Pat Waters is senior technician medicines management at Royal Wolverhampton Hospitals NHS Trust.
Correspondence to: Professor Fitzpatrick at Pharmacy Department, New Cross Hospital, Wolverhampton WV10 0QP (e-mail ray.fitzpatrick@rwh-tr.nhs.uk)
References
- Audit Commission. A spoonful of sugar: medicines management in NHS hospitals. London: Audit Commission; 2001.
- Department of Health. Pharmacy in the future — implementing the NHS plan. London: The Department; 2001.
- Slee A, Farrar K, Hughes D. Implementing an automated dispensing system. The Pharmaceutical Journal 2002; 268:437–8.
- Whittlesea C. What did research reveal about the effects of introducing automation? Hospital Pharmacist 2004;11:453.
- Slee A. Process and benefits of automation in hospitals. Hospital Pharmacy Europe 2004;(July/August):21–22.
- Swanson D. Automated dispensing — an overview of the types of systems available. Hospital Pharmacist 2004;11: 66–69.
- Fitzpatrick R. Implementing automation in a hospital pharmacy. Hospital Pharmacy Europe 2004;(March/April): 34–37.
- Fitzpatrick R. Automated dispensing — developing a business case to support investment. Hospital Pharmacist 2004;11:109–11.
- Department of Health. Medicines management in hospitals performance management framework. London. The Department; 2003.
- Department of Health. Vision for pharmacy in the new NHS. London: The Department; 2003.


