

Abstract
Aim
To ascertain the views of GPs in relation to their use of, and how they value, their local joint formulary.
Design
Questionnaire survey.
Subjects and setting
All 1,099 GP principals practising and employed by the 11 primary care trusts in the South West Peninsula Strategic Health Authority.
Results
Of the 470 respondents, 84% had their own hard copy of their joint formulary, and 34% had accessed their intranet formulary. 48% said they used their joint formulary to guide prescribing once a week or more, and 20% stated they referred to their joint formulary frequently to assist in the choice of drug therapy during individual patient consultations. Most GPs agreed that a joint formulary is a useful means of promoting consistent prescribing across the primary/secondary care interface, and that their approach to prescribing had been influenced by, and had improved since, its introduction. 93% agreed that their joint formulary has an educational value attached to it, and 87% welcomed feedback on adherence to the joint formulary. Only 39% had noticed any influence of the joint formulary on hospital prescribing. Free text comments to open questions on the joint formulary concept and how formularies should develop were broadly positive although some GPs did express negative views.
Conclusions
Overall GPs’ comments on their joint formularies were positive especially around the educational value of such a document and the potential for improving prescribing across the interface. However there were concerns from GPs about how the formulary is actually implemented and followed within secondary care.
Prescribing formularies have been in existence for many years as separate entities in both primary1 and secondary care.2 It is clear that if GPs and their local hospital relate to different and independently developed formularies then there is the potential for confusion around prescribing choices, patient harm and waste of NHS resources. Lack of continuity in prescribed medicines when patients are admitted into, and discharged from, hospital is a recognised problem. In addition, hospital prescribing has a significant impact on GP prescribing3,4 and GPs sometime express concern over recommendations originating from secondary care.
Although a number of notable joint formularies have been in existence for some years,5,6 the concept of a joint formulary is now attracting much more attention.7 Changes in the NHS, placing primary care on the same footing as secondary care and unifying their financial arrangements, have been a stimulus to the concept of combined formularies. Whole system prescribing arrangements, including joint formularies, have been officially recommended.8,9 A 2003 national survey of 223 primary care organisations revealed that just under half were already working with their local hospitals to achieve agreement around which drugs will be used in the local healthcare economy.10
The local health communities in the south west peninsula (Devon, and Cornwall & Isles of Scilly) started developing joint formularies for prescribing at least five years ago. Across the peninsula there are now five main joint formularies in existence, each one having been developed between the five distinct health communities of primary care trusts (PCTs) and acute trusts.
There have been slightly differing approaches to developing these formularies, and there are some minor differences in layout and format. However, incorporating GPs’ views so as to encourage ownership rather than imposition11 has been an essential part of the process in all health communities. These formularies have been designed as an advisory tool to promote evidence-based, safe, cost-effective prescribing across the health communities. Although the formularies are not prescriptive, they have been developed and promoted with the aim of covering about 80 per cent of prescribing, acknowledging that there will be instances where prescribing outside the formulary will be both necessary and appropriate.12
Adherence to formularies in terms of choice of drug as well as when to use drug therapy should enhance the efficiency of GP prescribing — a national and local imperative. The formularies are also seen as tools for promoting national guidance such as that from the National Institute for Health and Clinical Excellence and national service frameworks, as well as identifying clinical governance issues. Formularies are also intended to reflect and uphold the movement towards evidence-based medicine, and may assist medical practitioners in responding to the large volume of information delivered to them by the pharmaceutical industry.13 In the UK, evaluation of the impact of GP formularies has been reported at practice level14 and at primary care organisation level,1 and the views and perceptions of GPs to the formulary concept have been described.15,16 However, the evidence base of the impact of GP and primary care formularies is rather weak.17 Although joint formularies now have official support, the evidence base for their effectiveness in changing prescribing behaviour in primary care is also limited,18 and there is a lack of published information describing how GPs perceive joint formularies.19,20
Each of the five health communities produces a paper version and an electronic version (accessible via the local NHS intranets) of their joint formulary. Although each health community continuously monitors prescribing by use of prescribing analysis and cost data, robust evaluation of the impact of the joint formularies in terms of guiding drug choices, and how GPs feel about the joint formulary concept, has been lacking. The main aim of our study was, therefore, to investigate the impact that these formularies have had on GP prescribing.
The study combined a mixture of quantitative research (a questionnaire survey of GPs and evaluating prescribing trends for particular drug groups) and qualitative research (focus group interviews with formulary committees). It is the results of the GP questionnaire survey that are reported here.
The aims and objectives of this aspect of our study were to elicit the views of GPs in relation to their use of, and how they value, their local joint formulary, to understand how they make use of these documents in their routine practice and how they see joint formularies developing in the future.
Method
A brief survey instrument (four sides of A4, including a covering letter) was developed consisting mainly of closed questions, some of which required responses on a four-point Likert scale. In the main, these closed format questions either quantified the choices so as avoid differing interpretations, or asked for one of four answers to be given: strongly disagree, disagree, agree, strongly agree. A separate section, with four main headings, allowed for free text comments. These heading examined the general concept of the joint formulary, layout of the documents, their future development, and views on supporting information contained in the joint formulary. This questionnaire was piloted on a small number of GPs and minor modifications were incorporated.
The questionnaire and a return postage prepaid envelope were distributed via NHS courier during November 2004 to all 1,099 GP principals in the five health communities, with surgery addresses having been obtained from the respective PCTs. Questionnaires were completed anonymously. Quantitative data were entered into Microsoft Excel 1997, and responses to open questions were entered into a text file before major themes were analysed. Non-responders were not followed up. The study was not designed to compare data across the various health communities. Ethics committee approval was granted for the study.
Results
Responses were received from 470 of the GPs surveyed (42.8 per cent). Not all GPs answered all the questions and thus some totals do not add up to 100 per cent.
Of the respondents, 11 per cent had seen a copy of their formulary but did not have a personal copy, 84 per cent had their own hard copy, and 3 per cent claimed to be unaware of the existence of such a document. Just under half (48 per cent) were aware of its existence as an electronic document on the intranet but had never used it, 34 per cent had accessed the intranet formulary and 18 per cent did not know it existed. Nearly two-thirds of GPs preferred to use the paper version and 15 per cent preferred to use the electronic version.
Forty-eight per cent of respondents said they used the joint formulary to guide prescribing in general once a week or more, 26 per cent at least once a month, 10 per cent less than once a month and 15 per cent rarely. When asked how often they referred to the joint formulary to assist in the choice of drug therapy during individual patient consultations, 20 per cent stated that they do this frequently, 59 per cent occasionally, and 20 per cent responded that they did not use it at all.
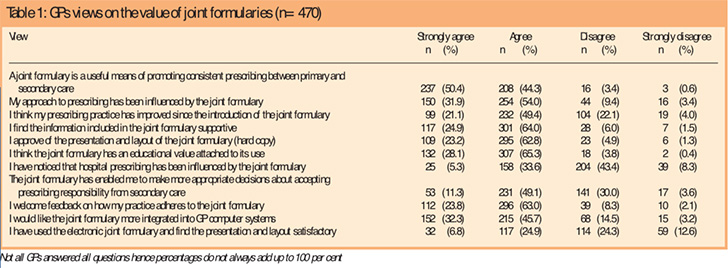
The questionnaire then asked GPs to rate their agreement with a number of statements (ranging from strongly agree to strongly disagree) relating to prescribing across the interface, their own prescribing practice, and the content, layout and educational value of their joint formulary. The results are shown in Table 1, from which it can be seen that 95 per cent of GPs agreed that a joint formulary is a useful means of promoting consistent prescribing across the interface, and 86 per cent agreed that their approach to prescribing had been influenced by the formulary. Seventy per cent of GPs agreed that their prescribing practice had improved since the introduction of the formulary, 93 per cent agreed that the formulary has an educational value attached to it, and 87 per cent welcomed feedback on their adherence to the formulary. In terms of secondary care prescribing, only 39 per cent had noticed any influence of the formulary on hospital prescribing.
Free text comments were then invited on specific aspects of their joint formulary although not all respondents expressed a view. Comments relating to the concept of a joint formulary (for examples see Panel 1) were received from 225 GPs (20 per cent) and were in the main broadly positive, with 78 per cent of the comments using descriptive words such as “good”, “excellent” and “essential”.
Panel 1: Comments on the general concept of the joint formulary
Broadly positive views
- Excellent, really useful in daily GP work
- Essential as long as not compulsory — we all have our own favourites that aren’t in the formulary
- A guide rather than a BNF replacement
- Excellent, encourages co-operation, compliance and good practice between primary and secondary care
- Essential to a seamless primary/secondary care interface — has done more than anything else to promote dialogue on prescribing
- Good idea but secondary care frequently undermines it by telling patients to come to us for non-formulary drugs and prescribing off licence — also secondary care does not await formulary development
Broadly negative views
- In the 10-minute slot I have too much to do without referring to a guide
- I feel decisions are made by price not effectiveness
- Far too narrow a choice, usually out of date and slow to take on innovative treatments
Major themes included the value of the joint formulary as an educational tool and a guide for prescribers. Ten per cent of the comments described an apparent lack of engagement with the joint formulary by hospital prescribers, but pointed to the valuable role that a joint formulary could potentially contribute to harmonising primary and secondary care prescribing. Less than 10 per cent of the comments could be categorised as broadly negative. These included disagreement with the joint formulary concept, concerns that such a document should not be seen as prescriptive, suggestions that low drug cost was the only reason for inclusion in the formulary (six comments), or questions how using such a document could be integrated fully into the time allowed for a patient consultation.
There were 198 free text responses on the presentation and layout of the joint formularies; again, these were broadly positive. Negative views related to poor indexing of the paper version (nine comments) and inaccessibility or difficulty in navigating the electronic versions (19 comments).
One hundred and ninety-two GPs provided comments about future developments to the joint formulary (for examples see Panel 2).
Panel 2: Comments on how GPs think the joint formulary should develop in the future
- Included in all computer programs, integration with GP prescribing software
- Continual updating useful, paper copy to be small and concise, electronic with links to further info — guidelines, evidence etc
- Keep it simple and as small as possible; the bigger it gets the less I will use it
- Audit formulary adherence at GP and hospital level
- I often turn to use the BNF for warnings, safety advice, dosage, side effects, and perhaps some of this could be in the formulary
- More advice on how to avoid inappropriate use of drug whether or not in formulary
- Just stop it and leave GPs to make their own decisions!
One major theme was the wish to see the joint formulary incorporated into prescribing support software (15 per cent of responses). GPs were keen to see the joint formulary updated regularly with the inclusion of additional guidance and reflecting recent research. Other comments again identified the need for improved use of the joint formulary by secondary care (16 per cent of responses), and the possibility of monitoring adherence to the joint formulary. A few GPs questioned the need to replicate the British National Formulary.
One hundred and twenty-five GPs commented on the supporting information contained with the joint formulary and were broadly supportive of additional information (such as asthma guidance) and summaries of, and links to, NICE guidance. A number of respondents stated that they refer to the BNF for more detailed information.
Discussion
The results of this survey demonstrate that GPs were generally positive about the joint formulary concept, the way the information was presented to them, and the effect that such guidance and advice had had on their prescribing. Just less than half the surveyed GPs responded, but this study provides valuable information for those involved in developing joint formularies. Between 70 and 95 per cent agreed that a joint formulary is a useful means of promoting consistent prescribing across the interface, that their approach to prescribing had been influenced and improved by the formulary, and that the formulary has an educational value. Such a shared approach will help in overcoming the inefficient care resulting from a lack of consistency and co-operation between primary and secondary care.21 The educational benefits of formularies have previously been discussed,22 accepting that, of themselves, they do not produce rational prescribing.
Improving both quality of treatment and the continuity of health care are important topics. Guidelines (in this instance the joint formulary) are one of the means to reduce variation and promote consistent prescribing, especially for patients with chronic conditions who often need care from both sides of the primary and secondary interface. In the main GPs considered themselves to be supportive of the joint formulary concept but they expressed recurring concerns over the implementation of the joint formulary in secondary care, as illustrated elsewhere.23 Likewise, others have reported that specialists do not perceive the same need for joint guidelines as do GPs19 and that formularies can be viewed as too restrictive24 — these may be barriers to the implementation process in hospitals. Organisational policies and procedures, as well as enforcement, can increase adherence to guidelines.25
Eighty-seven per cent of our GPs stated that they would welcome feedback on their prescribing patterns, an important component in achieving good adherence to a formulary. A minority of GPs, however, in their free text comments, expressed concerns over loss of clinical freedom and the threat that joint formularies would become mandatory and too focused on driving down prescribing costs. GPs were enthusiastic for the joint formulary to be incorporated into their prescribing support software as a future development, yet previous studies have identified making time during consultation for use of such systems as a significant obstacle and an impediment to the implementation of primary care guidelines.26 A small number of our GPs held similar views around this lack of time within a consultation to use a formulary document, with others suggesting ways that might improve the value of such a document, eg, better indexing and cross-referencing of drugs.
Other research into joint formularies is limited and conflicts with our results. Shaw and Wright20 reported that, although primary and secondary care stakeholders were aware of the existence of a joint formulary, not all were aware of its contents. In their study, adherence to the formulary was low as was belief in its effectiveness. However, stakeholders’ views were sought only 18 months after introduction of the joint formulary and this may have been too soon for active and adequate promotion of the formulary. Aström and colleagues16 noted that around three quarters of GPs believed local guidelines were necessary for cost-effective prescribing and good prescribing, but only 38 per cent admitted using the local guidelines (not necessarily joint formularies) more often than monthly. In our study just under half the respondents said they used the joint formulary to guide prescribing once a week or more.
There are a number of limitations to this study. The response rate of only 43 per cent is on the low side for GP studies27 and means that we are unsure if the positive comments and opinions expressed here are generalisable to the wider population of GPs in the peninsula. Non-responders may not consider the joint formulary to be a priority and may be uninterested in the concept. Major themes mentioned as free text comments include some which were potentially led by the statements used for the Likert scale and, therefore, were possibly not freely expressed views.
However these are themes that one would expect to arise in any discussion with GPs about joint formularies. Habitation, whereby the same response is given to a series of questions that have the same answer choices, is a recognised problem with questionnaires. Although open format or free text questions, of which we had four, have their advantages, they also have disadvantages in that they require more thought and time on the part of the respondent. Whenever more is asked of the respondent, the chance of tiring or boring the respondent increases, and this may be the reason why only one-quarter to one-half of respondents answered these questions.
A common problem in questionnaire surveys is the tendency of people to give socially desirable answers. We tried to limit this by emphasising that the data would be processed anonymously thus it was not possible to link responses to demographic details of the respondent. We cannot investigate, therefore, if there were differing rates of response between, for example, dispensing and non-dispensing practices or older and younger GPs.
This study researched the behaviour and attitudes of GPs towards their joint formulary. A quantitative study looking at the impact of the joint formulary recommendations on actual prescribing data is the subject of another report. It is acknowledged that outcomes such as actual patient benefits were not measured in this study. However, there is the expectation that if prescribers in both primary and secondary care do implement and follow recommendations in a joint formulary then improved continuity of care, cost-effective prescribing and safer prescribing should result.
This survey has elicited the extent of use, type of use, criticisms and suggestions for how the joint formulary concept can improve and will be of value to the various formulary committees operating throughout the peninsula.
Acknowledgements
This study was funded by a Plymouth Teaching PCT Small Project grant.
This paper was accepted for publication on 23 January 2006.
About the authors
Sarah-Jane Heal, MRPharmS, is lead formulary pharmacist at West Herts Hospital NHS Trust (at time of study, joint formulary pharmacist, Plymouth Teaching Primary Care Trust). Nicola Challinor is prescribing analyst, Plymouth Teaching PCT.
Chris Roome, MRPharmS, is interface development pharmacist, Royal Devon and Exeter Hospital Foundation Trust.
Shivaun Gammie, PhD, MRPharmS, is strategic pharmaceutical adviser and Julian Thorne, PhD, MRPharmS, is formulary pharmacist at Torbay Care Trust.
Michael Wilcock, MRPharmS, is head of the prescribing support unit at Central Cornwall PCT.
Correspondence to: Michael Wilcock, Pharmacy Department, Royal Cornwall Hospitals NHS Trust, Truro TR1 3LJ (e-mail mike.wilcock@centralpct.cornwall.nhs.uk).
References
- Hill-Smith I. Sharing resources to create a district drug formulary: a countywide controlled trial. British Journal of General Practice 1996;46:271–5.
- Petrie JC, Scott AK. Drug formularies in hospitals. BMJ1987;294:919.
- Audit Commission. A prescription for improvement. Towards more rational prescribing in general practice. London: HM Stationery Office; 1994.
- Greenfield SM, Jones MI, Stevenson FA, Nayak A, Bradley CP. General practitioners and hospital-initiated prescribing. European Journal of General Practice 2001;7:18–22.
- Garvey G. Grampian Health Board’s joint drug formulary. BMJ1990;301:851–2.
- Beard K, Forrester E, Lee A, Burns H, Brodie MJ. Systems and strategies for managing the drugs budget in Scotland. BMJ 1998;317:1378–81.
- Duerden M, Walley T. Prescribing at the interface between primary and secondary care in the UK — towards joint formularies? Pharmacoeconomics 1999;15:435–43.
- Audit Commission. A spoonful of sugar. Medicines management in NHS hospitals. London: Audit Commission;2001.
- Audit Scotland. Supporting prescribing in general practice – a progress report. Edinburgh: Audit Scotland; 2003.
- Developments in formularies and prescribing lists in the local healthcare economy. Pharmacy Management. Available at: www.pharman.co.uk/cms/view.php/2979.html (accessed 23 January 2006).
- Conroy M, Shannon W. Clinical guidelines: their implementation in general practice. British Journal of General Practice 1995;45:371–5
- Barber N. What constitutes good prescribing? BMJ 1995;310:923–5.
- House of Commons Health Committee. The influence of the pharmaceutical industry. London: The Stationery Office; 2005.
- Avery AJ, Walker B, Heron T, Teasdale SJ. Do prescribing formularies help GPs prescribe from a narrower range of drugs? A controlled trial of the introduction of prescribing formularies for NSAIDs. British Journal of General Practice 1997;47:810–4.
- McGavock H, Wilson-Davis K, McGavock SA. Formulary revision: eliciting the opinions of users. British Journal of General Practice 1996;46:419–21.
- Aström K, Duggan C, Bates I. Influences on prescribing: the perceptions of general practitioners in two primary care trusts. International Journal of Pharmacy Practice 2002;10(suppl):R10.
- Do formularies work? Bandolier April 2002;98-5. Available at: www.jr2.ox.ac.uk/bandolier/band98/b98-5.html (accessed 23 January 2006).
- Stewart D, Milne K, Krska J, Downie G. Adherence to the Grampian joint drug formulary in general practice. Journal of Clinical Pharmacy and Therapeutics 1996;21:79–82.
- Kasje WN, Denig P, De Graeff PA, Haaijer-Ruskamp FM. Physicians’ views on joint treatment guidelines for primary and secondary care. International Journal for Quality in Health Care 2004;16:1–8.
- Shaw V, Wright DJ. Joint primary and secondary care formularies: opinions of stakeholders. International Journal of Pharmacy Practice 2005;13(Suppl):R74.
- Kvamme OJ, Olesen F, Samuelsson M. Improving the interface between primary and secondary care: a statement from the European Working Party on Quality in Family Practice (EQuiP). Quality in Health Care 2001;10:33–9.
- Essex B. Practice formularies: towards rational prescribing. BMJ 1989;298:1052.
- Murray M, Padfield PL, Maxwell SRJ. Does a hospital formulary influence prescribing practice in an acute medical admissions unit? Scottish Medical Journal 2005;45:76–9.
- Kwan J. Hospital formularies restrict evidence based practice. BMJ 2005;331:515.
- Ashford J, Eccles M, Bond S, Hall LA, Bond J. Improving health care through professional behaviour change: introducing a framework for identifying behaviour change strategies. British Journal of Clinical Governance 1999;4:14–23.
- Rosseau N, McColl E, Newton J, Grimshaw J, Eccles M. Practice based, longitudinal, qualitative interview study of computerised evidence based guidelines in primary care. BMJ 2003;326:314–21.
- Sibbald B, Addington-Hall JM, Brenneman D, Freeling P. Telephone versus postal surveys of general practitioners: methodological considerations. British Journal of General Practice 1994;44:297–300.


