Halfpoint / Shutterstock.com
After reading this article, you should be able to:
- Know the definition of hepatic encephalopathy (HE) and how it may develop in patients with liver cirrhosis;
- Describe how HE is diagnosed and know the differential diagnoses;
- Understand how HE is managed;
- Describe the role of the pharmacist in managing patients with HE.
Introduction
Hepatic encephalopathy (HE) is a life-threatening complication of cirrhosis1,2. In cirrhosis, hepatocellular failure of the liver prevents sufficient metabolism of toxins, such as ammonia. This leads to a build-up of ammonia in the blood, which eventually enters the brain and causes the cognitive symptoms that manifest in HE, as described below3. It is considered a frequent complication of cirrhosis — around 50% of cirrhotic patients will experience HE at some point during the disease4.
The rate of mortality is high following an episode of HE, with an estimated survival rate of 42% at year one and 23% at year three4. Treatment is primarily through hospitalisation, meaning the economic and clinical burden of the condition is considerable4.
Pharmacy professionals in primary and secondary care may offer medicines optimisation for patients living with cirrhosis to prevent the occurrence or recurrence of HE. Knowledge of common medications that could precipitate HE can be utilised to offer the most effective medication and dose, while also reducing the risk factors associated with the development of HE. Pharmacy professionals are well placed to offer advice about changing formulations of medications if the use of enteral tubes is necessary in the case of severe cognitive impairment or for nutrition. In the case of end-of-life care, pharmacy professionals can provide support in terms of rationalising medications and the use of anticipatory medications5.
This article provides an overview of the pathophysiology of HE, explores risk factors and the recognition of clinical symptoms, explains the grading and diagnostic process for the condition, and outlines best-practice approaches to pharmacological management.
Pathophysiology
The mechanism behind the neuropsychiatric symptoms related to HE is not fully understood. However, it is established that raised ammonia concentrations play a role6,7. Cognitive symptoms, such as delirium in the absence of a raised ammonia level, will often rule out HE. However, symptoms of HE may still be present in the absence of raised ammonia owing to other contributing factors involved in the pathophysiology of HE, such as swelling of the brain, which is often visible on magnetic resonance imaging6,8.
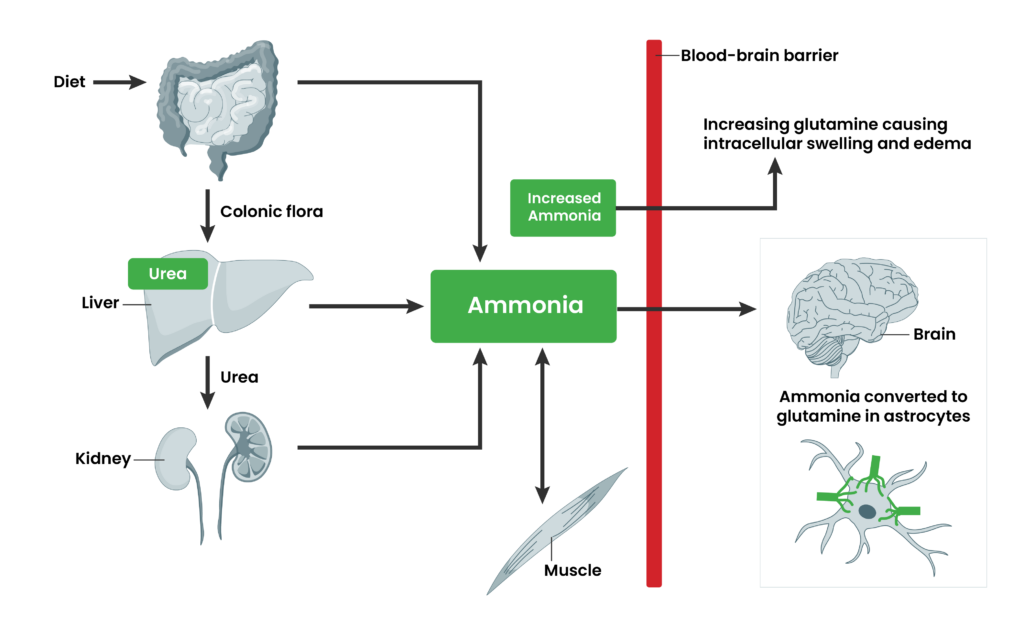
Protein taken in the diet is broken down to form ammonia, which then enters the liver where it would normally be metabolised via the urea cycle (see Figure 18,9). In liver cirrhosis, hepatocellular damage decreases the function of the urea cycle and causes excess ammonia to enter the systemic circulation. This ammonia crosses the blood–brain barrier and is converted to glutamine in the astrocytes. This leads to osmotic effects whereby excess water results in the swelling of the astrocytes and causes neuropsychiatric symptoms related to HE, including cerebral oedema and cytotoxic brain injury7,8.
Figure 1: The role of ammonia in hepatic encephalopathy
Signs and symptoms
Common symptoms of HE include:
- Changes in personality, such as behavioural change, irritability, agitation, anxiety, apathy and euphoria;
- Short-term memory loss;
- Disorientation;
- Asterixis (i.e. tremor of the hands);
- Confusion and loss of concentration;
- Lethargy;
- Ataxia (i.e. difficulty with balance, walking and speech);
- Slurred speech;
- Altered sleep–wake cycle (i.e. sleeping throughout the day and remaining awake all night);
- Somnolence (i.e. excessive drowsiness, sleepiness);
- Coma2,7.
Alongside the symptoms related to HE, signs that indicate its presence may include:
- Raised serum ammonia;
- Established diagnosis of liver cirrhosis;
- Other symptoms related to chronic liver disease, such as jaundice, ascites, presence of varices and other biochemical and image-related observations10.
The signs and symptoms related to HE are potentially reversible, dependent on the precipitating factors described below.
Risk factors and precipitating events
Common precipitating factors for the development of HE include sepsis and inflammation, electrolyte disturbance, dehydration, gastrointestinal bleeding, constipation and use of some medications1.
Decreased ammonia excretion owing to constipation and renal impairment can precipitate symptoms of HE. Use of certain medications that may cause constipation (e.g. sedatives, opioids) or that may cause renal impairment and electrolyte imbalances (e.g. diuretics) are also risk factors for the development of HE7. Different electrolyte disturbances give rise to different complications associated with HE but are beyond the scope of this article. Further information on this topic can be found here11.
Paracentesis should be performed with caution with patients at risk of HE. During paracentesis, ascitic fluid is removed from the abdominal cavity, which may give rise to post-paracentesis circulatory dysfunction. The use of Human albumin solution (HAS) should be readily available to mitigate this risk. Post-paracentesis circulatory dysfunction may lead to renal impairment and exacerbate HE, which in some cases can be fatal12,13.
What are the different types of HE and how is it graded?
Hepatic encephalopathy can be subdivided to overt HE (OHE) and minimal (i.e. covert) HE (MHE)7. Grading of HE is used to identify the severity of symptoms and is graded 0-4 using the West Haven criteria for defining the severity of HE7,14. Minimal HE is defined by grade 0-1 of the West Haven criteria14, while diagnosis is primarily done using neuropsychological testing7,14. See Table 1 for more information on the different grades of HE along with a description of the symptoms7.
Table 1: West Haven criteria for defining the severity of hepatic encephalopathy
Diagnosis
Diagnosis of HE can be complex as no single investigation can confirm it7. A combination of effective history taking, clinical examination and other investigations all play a role in determining the diagnosis of HE1.
Many of the symptoms of HE can be commonly related to other conditions with cognitive manifestations, including coma. It is important to rule out such causes. Investigations may be used to aid this — for example, an electroencephalogram may be used to rule out confusion related to epilepsy. A head CT may be used to rule out subdural haematoma, intracranial bleeding, stroke, cerebral infarctions or tumours7. An effective history will ensure any possible precipitants of HE are identified — for example, overuse of opioids leading to constipation and symptoms of HE.
Neuropsychological tests — such as the five-point star, number connection and animal naming — can be used to diagnose minimal HE, grade 0-1. However, overt HE cannot reliably be diagnosed using these tests. Serum ammonia is useful for the diagnosis of HE as a large proportion of patients will have raised ammonia levels7. However, it is not vital if other symptoms overwhelmingly support HE as the diagnosis, such as existing risk factors, asterixis and drowsiness7.
The possibility of sepsis-related symptoms can be ruled out by investigating blood tests, blood cultures, urinalysis, chest X-ray and an ascitic tap if ascites is suspected7. Other causes for encephalopathy should also be ruled out — for example, Wernicke’s encephalopathy in the case of acute thiamine deficiency often related to excess alcohol intake; toxic encephalopathy related to certain drugs such as sedatives; and metabolic encephalopathy related to hypoglycaemia, diabetic ketoacidosis and hypoxia7.
Management
The aim of HE management is ultimately to avoid progression to overt HE, as well as the development to coma and death.
The British Society of Gastroenterology (BSG) has set out clear guidance for the management of HE15. Treatment should begin by identifying the cause of the HE and treating that, as well as offering the patient other licensed, and sometimes unlicensed, forms of therapy. Treatment for HE should always involve specialist hepatology teams and admission to hospital is required.
See Figure 2 for a useful flow diagram from the BSG, outlining the treatment steps for a patient presenting with overt HE symptoms15.
Figure 2: BSG guidance for the management of overt HE
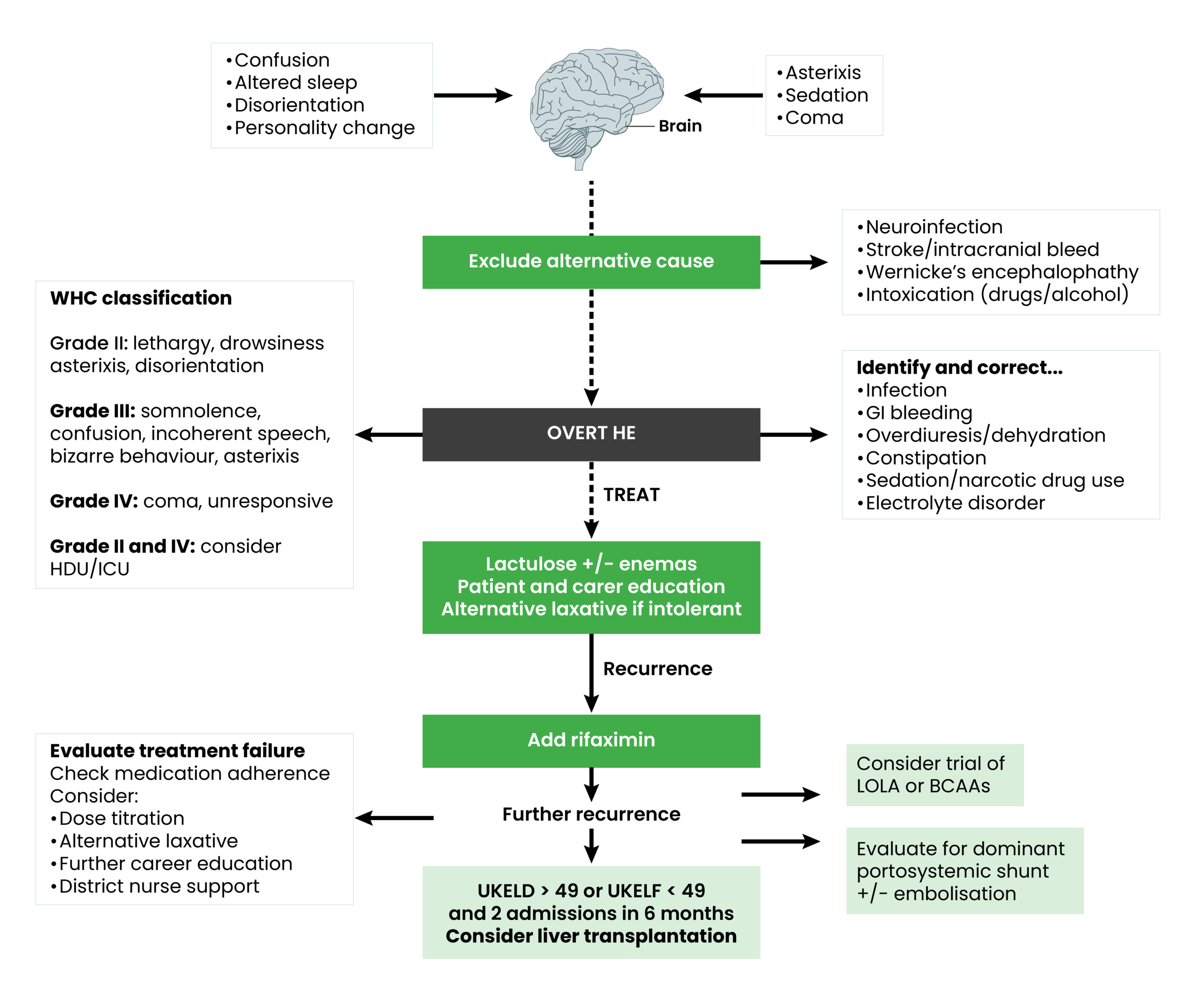
Lactulose is licensed in the UK for the treatment of HE16. Its mechanism of action works by reducing the production and absorption of ammonia in the gut. Starting doses are usually higher than for treating constipation. A starting dose of 30ml three times daily with the aim of ensuring two to three bowel motions per day16 is common. Patients are advised to adjust the dose as per bowel motions. However, in the authors’ experience, compliance may be an issue for some patients given some of the side effects of lactulose, such as increased flatulence, bloating, nausea and a sweet taste that can often be described as sickly. Adherence to treatment can be a reason for HE recurrence. Regular reviews with healthcare professionals should address issues surrounding compliance. Introduction of structured education tools are in use to address this and other aspects of patient education15. Contraindications for its use include gastrointestinal perforation16. Alternatives to lactulose would be the use of enemas, such as phosphate enemas. However, these can be impractical and are often associated with pain17.
If HE persists, despite regular use of lactulose, treatment should be escalated to include the concomitant use of rifaximin. Rifaximin is an oral therapy and works similarly to lactulose by reducing the absorption and production of ammonia, delaying the occurrence of acute episodes of HE. It is technically an antibiotic that alters the function of the gut flora. However, rifaximin is not associated with antibiotic resistance18. Trials have demonstrated positive outcomes when used in combination with lactulose, including reduced overall mortality from HE, improved symptoms of HE and prevention of recurrence, and has demonstrated shorter lengths of stay in hospital because of its use18. Common side effects include headache, nausea and vomiting, oedema and low mood. Contraindications include intestinal obstruction19.
Even when used together, lactulose and rifaximin may not reduce symptoms of HE. Therefore, clinicians may explore other therapies that are not licensed in the UK. L-ornithine L-aspartate (LOLA) is an agent used commonly by hepatology clinicians for this indication. It is licensed for use in Europe and classed as a medical food in the United States. However, it is currently not licensed in the UK20.
LOLA is indicated for ammonia detoxification in overt and minimal HE in resistant, recurring HE that usually results in hospital admission. It works by stimulating ammonia detoxification in the liver and muscle via the activation of the urea cycle and glutamine synthesis, respectively21.
The results of a meta-analysis of randomised controlled trials, published in 2019, revealed evidence of the benefit of LOLA22. This included improvement of mental state grade in OHE and MHE. It demonstrated efficacy using both oral and intravenous formulations of LOLA. There is also evidence of head-to-head trials comparing the efficacy of LOLA with other ammonia-lowering agents, such as lactulose and rifaximin, showing LOLA is equivalent and, in some cases, superior to alternative agents15,23. However, concerns over the quality of evidence were noted in one meta-analysis. These included use of different terminology for the different grades of HE and it is proposed that larger randomised controlled trials (RCTs) are required for better quality of evidence22. The findings of network meta-analyses showed that LOLA appears to be comparable — or superior — in efficacy to non-absorbable disaccharides (e.g. lactulose) or probiotics. Emerging evidence from single RCTs show efficacy of LOLA for the treatment of post-trans-jugular intrahepatic portosystemic shunt (TIPSS) HE, as well as for secondary HE prophylaxis22. These findings provide support for the use of LOLA in the treatment of HE and suggestion is made for future trials focusing on the use of LOLA for prophylaxis.
LOLA is contraindicated in severe renal impairment (serum creatinine of >265 micro-mol/L)21. However, side-effect profiles remain satisfactory, with headache and nausea being the only common ones reported21. Dosing information from the manufacturer recommends one to two sachets of LOLA one to three times per day. However, higher doses can be used as per the patient presentation, with no information for maximum doses available21.
Branch-chain amino acids (BCAAs) have a place in therapy for the reoccurrence of overt HE, despite previous use of lactulose and rifaximin in patients who are not eligible for transplant15. Their mechanism of action involves supplementation of amino acids to ensure conversion of ammonia to glutamine in the skeletal muscle; therefore causing its detoxification and reducing the symptoms of HE15. There are no head-to-head trials that compare the efficacy of BCAAs; therefore, use in practice is low15.
Best practice for pharmaceutical care for the HE patient
Pharmacists and pharmacy teams are often regarded as experts in dealing with medications. In the case of HE, they play a role in the management of the patient during admission and on discharge from hospital. Discussion with the wider multidisciplinary team is often useful in optimising the patient’s medications relating to withholding, deprescribing or reducing the doses of precipitant medications, such as those seen in Table 224.
During the diagnostic phase, it is important to identify possible risk factors for the development of HE. A review of the patient’s medications prior to admission — prescribed and bought over the counter — should be evaluated. Common medications to consider include those that may reduce normal bowel movement and result in constipation. Table 2 below gives some common examples of medications that may cause constipation24.
Table 2: Examples of medicines that can cause constipation
Sedative medications can contribute to cognitive decline and exacerbate symptoms of HE — examples include benzodiazepines (e.g. chlordiazepoxide, lorazepam, diazepam, zopiclone), opioid medications (codeine, tramadol, morphine) and tricyclic antidepressants (e.g. amitriptyline)15.
Although diuretics are required in the management of the cirrhotic patient, usually for ascites, they may also result in dehydration and electrolyte disturbances, which can exacerbate the symptoms of HE15.
Overuse of paracetamol, even within the maximum daily dose, may be detrimental to the cirrhotic liver and exacerbate HE symptoms.
Pharmacy professionals may work with the clinical team to provide support in end-stage liver failure by rationalising medicines that may not be a priority in the last few days and weeks of life, as well as advising those medicines that would be appropriate to ensure comfort for the dying patient5.
Depending on the extent of cognitive impairment, patients with HE may require alternative feeding options, such as nasogastric (NG) tubes. Pharmacy teams can provide information regarding changing to the most appropriate formulation or manipulating the medication to allow for enteral tube feeding, such as crushing tablets, which would be used on an off-label basis.
Pharmacists can support clinical teams in providing the best management as per local and national guidelines. Utilisation of other pharmacy colleagues to ensure availability of the medication can ensure the patient receives the medication efficiently to prevent further development of HE and thus reduce lengths of stay in hospital.
Provision of some medications may not be readily available. LOLA is an unlicensed medication that is only available from Europe. Such medications may require special authorisation from pharmacy medicines optimisation groups — or equivalent — to ascertain the safety, cost-effectiveness and suitability for the use of the medication within the trust. Knowledge of such systems and processes is necessary to ensure availability of the medication. Ensuring effective communication with pharmacy procurement teams and knowledge of delivery dates/times is required. Educating prescribing colleagues on new medications, as well as on the development and implementation of local guidelines, is good practice. It is often needed in such circumstances to ensure safe prescribing. Pharmacists are best placed to provide this specialist service for clinical colleagues and, ultimately, the patient.
Review of stable patients is necessary to avoid overuse of expensive medications. Rifaximin can often be deprescribed if patients no longer present with HE symptoms over a long period. Regular audits of costly medications are good practice to keep to NHS budgets and prevent patients from taking medications that may not be required.
Educating patients to be aware of the more subtle symptoms of HE and informing carers is useful in preventing overt HE symptoms, which can result in hospital admission and death. Patients should be advised in methods to prevent some of the precipitants of HE, such as good compliance to treatment, avoidance of overuse of over-the-counter analgesia (e.g. paracetamol and codeine) and detecting the early signs of an infection15.
Summary
- HE is a complication associated with decompensated chronic liver disease. Manifestation of the neurocognitive symptoms associated with HE is mostly because of reduced detoxification of ammonia;
- Diagnosis involves ruling out of other causes of cognitive changes through effective history taking, medication history, and the use of various blood tests and imaging;
- HE can manifest in varying degrees of severity and can be recurrent. This can have a significant burden on patients, and their family or caregivers. The burden on the NHS remains high for such patients as treatment often requires access to secondary care;
- For this reason, it is important that patients, carers and healthcare professionals are aware of the common causes of the patient’s HE. Effective, structured education and frequent reviews can minimise this risk;
- Management of HE involves several options that are licensed and unlicensed. The aim of treatment is to identify the cause of HE, reducing the production and absorption of ammonia, and preventing recurrence;
- Pharmacists are well placed to provide some of this education and effective review of patients’ medications is an area where pharmacy professionals can benefit patients and may reduce the incidence of the recurrence of HE. This — alongside alcohol support services, often supported by pharmacy professionals — can play a role in reducing HE episodes among patients with a history of alcohol abuse25.
- 1.McPherson S, Abbas N, Allison MED, et al. Decompensated cirrhosis: an update of the BSG/BASL admission care bundle. Frontline Gastroenterol. Published online April 16, 2025:flgastro-2025-103074. doi:10.1136/flgastro-2025-103074
- 2.Clinical Knowledge Summaries (CKS). Cirrhosis, Background information, What is it? National Institute for Health and Care Excellence. 2024. https://cks.nice.org.uk/topics/cirrhosis/background-information/definition/
- 3.Hepatic Encephalopathy. Liver4life. 2019. https://www.liver4life.org.uk/hepaticencephalopathy
- 4.Cirrhosis in over 16s: assessment and management. National Institute for Health and Care Excellence. 2023. https://www.nice.org.uk/guidance/ng50/resources/cirrhosis-in-over-16s-assessment-and-management-pdf-1837506577093
- 5.Palliative management in end-stage liver disease. Pharmaceutical Journal. Published online 2018. doi:10.1211/pj.2018.20205508
- 6.Ritter J. A Textbook of Clinical Pharmacology and Therapeutics. 5th ed. CRC press; 2008. https://elearning.clinicalmedhub.com/pages/assets/file/medicine/A-Textbook-of-Clinical-Pharmacology-and-Therapeutics-5th-edition-1.pdf
- 7.Joshi D. Hepatology at a Glance. 2nd ed. Wiley-Blackwell; 2025. https://www.wiley.com/en-ie/shop/general-introductory-medical-science/hepatology-at-a-glance-2nd-edition-p-9781394217588
- 8.Tranah TH, Paolino A, Shawcross DL. Pathophysiological mechanisms of hepatic encephalopathy. Clinical Liver Disease. 2015;5(3):59-63. doi:10.1002/cld.445
- 9.Swaminathan M, Ellul M, Cross T. Hepatic encephalopathy: current challenges and future prospects. HMER. 2018;Volume 10:1-11. doi:10.2147/hmer.s118964
- 10.Mandiga P, Kommu S, Bollu P. Hepatic Encephalopathy. StatPearls; 2026. https://www.ncbi.nlm.nih.gov/sites/books/NBK430869
- 11.Jiménez JV, Carrillo-Pérez DL, Rosado-Canto R, et al. Electrolyte and Acid–Base Disturbances in End-Stage Liver Disease: A Physiopathological Approach. Dig Dis Sci. 2017;62(8):1855-1871. doi:10.1007/s10620-017-4597-8
- 12.What are the implications of paracentesis in patients with hepatic (liver) encephalopathy? Dr Oracle . 2025. https://www.droracle.ai/articles/71460/what-are-the-implications-of-paracentesis-in-patients-with
- 13.Large volume paracentesis in cirrhosis: safety toolkit. British Society of Gastroenterology. 2025. https://www.bsg.org.uk/getattachment/6fae5280-1796-4043-9cab-36b6455b5bca/Large-Volume-Paracentesis-in-Cirrhosis_Safety-Toolkit.pdf?lang=en-US
- 14.Mansour D, Masson S, Corless L, et al. British Society of Gastroenterology Best Practice Guidance: outpatient management of cirrhosis – part 2: decompensated cirrhosis. Frontline Gastroenterol. 2023;14(6):462-473. doi:10.1136/flgastro-2023-102431
- 15.Management of hepatic encephalopathy: beyond the acute episode. British Society of Gastroenterology. 2019. https://www.bsg.org.uk/web-education/management-of-hepatic-encephalopathy
- 16.Lactulose. National Institute for Health and Care Excellence. 2026. https://bnf.nice.org.uk/drugs/lactulose/
- 17.Sodium acid phosphate with sodium phosphate. National Institute for Health and Care Excellence. 2026. https://bnf.nice.org.uk/drugs/sodium-acid-phosphate-with-sodium-phosphate/
- 18.Zacharias HD, Kamel F, Tan J, Kimer N, Gluud LL, Morgan MY. Rifaximin for prevention and treatment of hepatic encephalopathy in people with cirrhosis. Cochrane Database of Systematic Reviews. 2023;2023(7). doi:10.1002/14651858.cd011585.pub2
- 19.Rifaximin. National Institute for Health and Care Excellence. 2026. https://bnf.nice.org.uk/drugs/rifaximin/
- 20.McAuley C, Clifford C, Smith A, Holt A, Rajoriya N. P79 Clearing the mind: LOLAs promise in hepatic encephalopathy- a real world experience. P79 Clearing the mind: LOLAs promise in hepatic encephalopathy- a real world experience. Published online October 2025:A67.1-A67. doi:10.1136/gutjnl-2025-basl.95
- 21.Hepa-Merz. Hepa-Merz. https://www.hepa-merz.com/hepa-merz/
- 22.Butterworth RF, McPhail MJW. l-Ornithine l-Aspartate (LOLA) for Hepatic Encephalopathy in Cirrhosis: Results of Randomized Controlled Trials and Meta-Analyses. Drugs. 2019;79(S1):31-37. doi:10.1007/s40265-018-1024-1
- 23.Fallahzadeh MA, Rahimi RS. Hepatic Encephalopathy: Current and Emerging Treatment Modalities. Clinical Gastroenterology and Hepatology. 2022;20(8):S9-S19. doi:10.1016/j.cgh.2022.04.034
- 24.Clinical Knowledge Summaries (CKS). Constipation, Background information, What are the secondary causes? National Institute for Health and Care Excellence. 2025. https://cks.nice.org.uk/topics/constipation/background
- 25.Community pharmacy: delivering substance misuse services. Office for Health Improvement & Disparities. 2024. https://www.gov.uk/government/publications/community-pharmacy-delivering-substance-misuse-services/community-pharmacy-delivering-substance-misuse-services