


Wes Mountain/The Pharmaceutical Journal
At a time of rising demand on the NHS and pressure on hospital appointments and space, homecare medicines services offer the chance to treat more people at home and save them the inconvenience of regular trips to hospital.
With around half a million people receiving homecare medicines services at a cost that is likely to be between £3bn and £4bn per year — there is little agreement about the precise figure — homecare is big business (see Box 1). But there are questions over what the NHS is getting for its money and how governance and accountability within the system could be improved.
Homecare medicines services typically involve the delivery, and sometimes administration, of expensive and complex medicines to patients in their homes. These could include medicines such as cancer therapies, biologics, enzyme replacement medicines, home parenteral nutrition, immunosuppressants and intravenous antibiotics. They often must be delivered as part of a “cold chain” and may need to be injected or infused.
The past year has seen rising concerns that homecare medicines services are failing patients, with a series of reports in the national media exposing how patients have been left without medicines or waiting weeks to start treatment[1–3].
In one incident, a patient died and three others were hospitalised after being administered incorrect amounts of an unlicensed version of the chemotherapy drug cabazitaxel manufactured as a ‘special’ by homecare company Sciensus (previously known as Healthcare at Home). Sciensus had its licence partially suspended by the Medicines and Healthcare products Regulatory Agency (MHRA) in July 2023 for a period of three months after an investigation found that the product was set up with the incorrect strength in the company’s IT systems. The suspension was subsequently extended for a further nine months because the deficiencies have not yet been fully resolved.
The House of Lords Public Services Committee opened an inquiry into homecare medicines services to investigate concerns in May 2023, which heard evidence from patient groups, regulators, homecare companies and the government during the summer[4]. Baroness Morris of Yardley, chair of the committee, pointed out during the last evidence session of the inquiry, in September 2023, that there seems to be a gulf between the views of patients, who feel the service is “awful”, and those of the providers, who feel it is “all fine”[5]. The committee will publish its report on 16 November 2023.
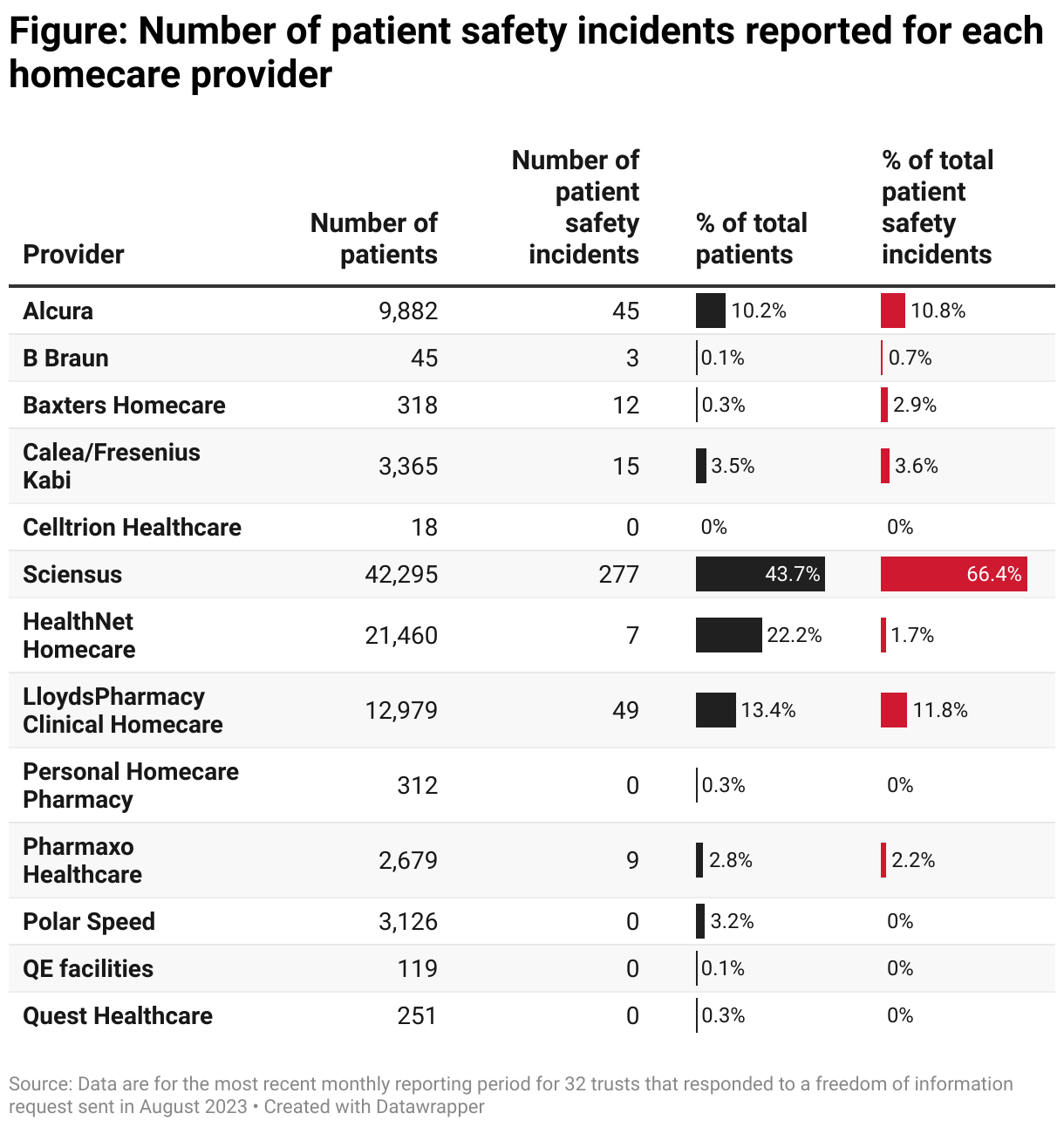
An investigation by The Pharmaceutical Journal has revealed that 32 trusts recorded 417 patient safety incidents relating to homecare medicines services provided to 96,846 patients during their most recent monthly reporting period, which ranged from May to July 2023. Some 66% of these incidents (277) related to services delivered by Sciensus, which provides homecare medicines to fewer than half (44%) of the patients covered in the data (see Figure). Where trusts gave figures for patient safety incidents over a 12-month period, this was divided by 12 to give a monthly average.
A patient safety incident is defined by the National Reporting and Learning Service as “any event that led to actual harm to a patient or had the potential to harm a patient”.
The data, released in response to freedom of information (FOI) requests sent by The Pharmaceutical Journal to 121 acute trusts and 10 specialist trusts in England in early August 2023, also uncovered that Sciensus was a poor performer on “failed” deliveries — those that did not arrive on the planned day. Among 34 trusts that used Sciensus to provide homecare for 48,237 patients and provided data about failed deliveries, on average they said that 8% of Sciensus deliveries failed. This was the highest average rate reported by trusts that gave us data on failed deliveries by different providers, with the rest ranging from 0–7%.
We believe it is crucial to ensure consistency in how incidents are reported
Spokesperson for Sciensus
“We work very hard to ensure people get their medicines on time and our patient services have a 95% satisfaction rating,” a spokesperson for Sciensus told The Pharmaceutical Journal. “Our clinical specialists, including our pharmacists, inform a clear policy of being open and transparent in reporting any incidents to ensure learning across all stakeholder groups.”
The spokesperson added that Sciensus would welcome an NHS review to ensure a common approach is adopted across the sector. “We believe it is crucial to ensure consistency in how incidents are reported, a view shared by patient groups who raised it in the recent House of Lords inquiry.”
HealthNet Homecare had the highest average rate of late deliveries — where the medicine arrived on the same day but not at the planned time. Among 34 trusts that used HealthNet to provide services for 23,423 patients and provided data on late deliveries, they said that an average of 16% of deliveries arrived late. The average rate for other companies ranged from 0–10%.
Chris Carver, deputy chief executive of HealthNet Homecare, told The Pharmaceutical Journal that the company is very strict about reporting “late” deliveries, which he said are classified as those not delivered within a two-hour timeslot, even if they are only a minute early or late.
“Where deliveries are outside the slot, over half were delivered early and 90% were within an hour of the slot,” he explains.
Box 1: How homecare medicines services are funded
Most homecare — somewhere between 70% and 80% — is paid for by pharmaceutical companies as part of their overall contract with individual hospitals, where they are paid a set amount to cover both the medicine and its delivery and administration, according to evidence given at the Lords Public Services Committee inquiry by Christian Selinger, consultant gastroenterologist and chair of the inflammatory bowel disease section at the British Society of Gastroenterology[6]. The delivery and administration are then often sub-contracted by the pharmaceutical company to a specialist clinical homecare provider, which is not guaranteed a particular volume of work.
This means the cost of homecare is particularly opaque — only in a few cases are the contracts “unbundled”, meaning the trust purchasing them can see what the cost of delivery and administration is. It is hard to see how much homecare providers are paid in this model, but it may mean they have tight margins and have struggled with inflationary pressures, especially around delivery staff and fuel.
Around 4% of homecare medicines services are commissioned directly by NHS England’s commercial medicines division, covering home parenteral nutrition, enzyme replacement therapy, lysosomal storage disorders, and pulmonary hypertension and bleeding disorders, Claire Foreman, director of medicines policy and strategy at NHS England, told the inquiry[7].
The remainder are commissioned directly by trusts, sometimes using regional frameworks arranged through procurement hubs, which allow trusts to “draw down” services as needed without going through further procurement processes.
There is some disquiet about the current model among pharmaceutical companies, which say they have little influence over which homecare company is chosen. According to the Association of the British Pharmaceutical Industry (ABPI), trusts are increasingly asking to have a say in which provider is chosen, often having arrangements in place with several different companies and insisting that one of them gets the contract for any new medicines added to its homecare services.
“There are three in this relationship,” says Rick Greville, ABPI director Wales Cymru and distribution supply chain. “The NHS, the homecare provider and the marketing authorisation holder.”
Pharmaceutical companies say they may not be aware when problems with homecare services are developing. There will be a service level agreement between the trust and several homecare providers, incorporating key performance indicators (KPIs), but information on achievement of the KPIs may not be shared with the marketing authorisation holder, says Greville.
UK-wide problems
Demand for homecare medicines services is increasing as more medicines become available[6].
Jennifer Allen, the chief pharmaceutical officer’s clinical fellow for 2022/2023, who is leading a refresh on the Royal Pharmaceutical Society’s (RPS’s) standards for homecare, says: “Homecare is growing exponentially, so there are large numbers of patients who have signed up to it.” The revised standards are out for consultation, but Allen says the existing ones are still “fit for purpose”[8].
It can take some patients weeks to get the first dose of the medicine that has been prescribed
Sarah Campbell, chief executive of the British Society for Rheumatology
Sarah Campbell, chief executive of the British Society for Rheumatology, which has brought together groups representing professionals and patients on the issue of homecare, says there are UK-wide problems with homecare medicines services that have been ongoing for some time. These range from lost or missing prescriptions through failed deliveries to delays in processing new patients and starting them on prescribed medicines.
It can take some patients weeks to get the first dose of the medicine that has been prescribed — and sometimes a patient’s condition may deteriorate during this time, or they may be left on drugs, such as steroids, which have side effects, explains Campbell. This delay can also impact on the efficacy of some drugs; for example, anti-tumour necrotising factor therapies have a better outcome for inflammatory bowel disease (IBD) when used early in the disease course, and patients can develop antibodies if they come off the drugs, which make them less effective when restarted. In severe cases, patients with IBD who are waiting to start medicines may end up in hospital, suggests Campbell.
Christian Selinger, consultant gastroenterologist and chair of the IBD section at the British Society of Gastroenterology, told the Lords Public Services Committee inquiry that the average time to wait between a clinician requesting homecare and services starting is around six to eight weeks[6]. With IBD patients, some trusts offer administration of the first one or two injections in hospital to avoid any delay.
Failed or delayed deliveries can cause considerable inconvenience for healthcare professionals too: the Lords Public Services Committee was told that 12% of 96 nurses who responded to a survey by Crohn’s & Colitis UK in May 2023 spent one day per week chasing up medicines[6].
The committee also heard from Ruth Wakeman, director of services, advocacy and evidence at Crohn’s & Colitis UK, that pharmacy services are spending up to 15 hours a week trying to resolve homecare issues for their patients[6].
Key performance indicators
Homecare companies are measured against several key performance indicators (KPIs), developed by the National Homecare Medicines Committee — which provides support for hospital chief pharmacists and has representation from the homecare industry, pharmaceutical manufacturers and NHS England’s commercial medicines unit — in 2013. The KPIs are published on the RPS website as an appendix to the Handbook for Homecare Services in England[9].
The Lords inquiry was told by Alison Davis, chair of the providers’ group, the National Clinical Homecare Association, that all hospitals get reports on KPIs monthly. There are 27 KPIs, which include the proportion of failed and delayed deliveries, as well as the number of patient safety incidents.
However, 37 of the trusts that responded to the FOI request told The Pharmaceutical Journal that they either do not hold data on the percentage of late and failed deliveries, do not hold them in a reportable form or it would take longer than 18 hours — the time limit for completing FOI requests — to collate the data.
There is currently no national publication of performance against KPIs, but Davis told the inquiry that 98.8% of deliveries in 2022 were on the day they were intended for.
The position is further muddied by there being no set target for achievement of the KPIs, making it hard to define what is a “good” service or say whether a provider is “failing”.
Regulation of homecare services is fragmented (see Box 2) and there seem to be no penalties for providers that miss KPIs. Any challenges experienced may be discussed at meetings of the National Homecare Medicines Committee supplier engagement subgroup, but the committee cannot enforce any action as a result of those discussions.
One homecare company told The Pharmaceutical Journal that it would welcome clarification of the existing KPIs and therefore greater consistency in reporting, especially around indicators such as patient safety incidents.
Campbell wants to see performance against KPIs made public.
NHS England is carrying out a “desktop exercise” to understand how governance and accountability work in the homecare sector. David Webb, chief pharmaceutical officer for England, told the Lords Public Services Committee that the exercise may lead to additional investigations. He also said that the National Homecare Medicines Committee is consulting on a new raft of KPIs, on which it will attempt to publish provider’s performance against at a national level[5].
NHS England did not respond when The Pharmaceutical Journal asked for more details of the desktop exercise.
Box 2: Regulation and accountability
A trust’s chief pharmacist will be “individually responsible for the services that are provided to patients”, according to David Webb, chief pharmaceutical officer for England, who gave evidence at the House of Lords committee inquiry into homecare medicines services[7]. There is support from regional specialists, but Webb admitted that “the local support to manage these contracts effectively is limited”.
Regulation is also complicated. The General Pharmaceutical Council has a role in terms of regulating registered pharmacy premises and the pharmaceutical services they deliver but the Medicines and Healthcare products Regulatory Agency (MHRA) and the Care Quality Commission (CQC) also have a regulatory role. Any service that has a nursing element will need CQC regulation or its equivalent in Scotland and Northern Ireland. And the MHRA will regulate any company which makes compound and licensed medicines (such as some chemotherapies) or does wholesaling activity.
Potential solutions
Digitalisation of prescriptions is seen as crucial to improving homecare services, with Webb telling the Lords Public Services Committee that “digital interoperability is absolutely essential”[7].
Data from the 2023 NHS Benchmarking Network pharmacy and medicines optimisation project show that only 3 trusts reported 100% of homecare medicines are prescribed electronically and 55 trusts reported that 0% of homecare medicines are prescribed electronically. Digitalisation could streamline the system and reduce some of the administrative burden, including on hospital pharmacies and among homecare providers. It would also ensure an audit trail and get rid of any “lost in the post” issues.
However, from a homecare provider perspective, there is no national secondary care IT system in the NHS, with trusts using an array of systems. This creates challenges with interoperability, despite the existence of core standards across the NHS.
There will also need to be investment in hospital pharmacy homecare teams. The National Clinical Homecare Committee, which declined a request to speak with The Pharmaceutical Journal, proposed in 2021 that commissioners should pay a levy of between £90 and £234 per patient to help cover the costs that homecare imposes on trusts — even when the medicines are delivered by a third party[10]. It has also suggested that small trusts could work together to reduce costs.
I’m sure we could work more closely with homecare companies to bridge that gap
James Allen, chief pharmacist at University Hospitals Southampton NHS Foundation Trust
James Allen, chief pharmacist at University Hospitals Southampton NHS Foundation Trust, says that homecare requires dedicated resources aligned to patient numbers. However, he believes that, once the service is established, it does not pose too much of an additional burden on the department and the flow of information about performance is generally good.
“Resource wise, the entire process of using homecare is probably not that different from if we were supplying the medications ourselves, but it does require resources, oversight and a team with the appropriate skill mix,” he says.
But he adds there can be periodic challenges and he may not always hear about a problem as quickly as the homecare company does, and that these delays in communication can lead to additional work. “I’m sure we could work more closely with [homecare companies] to bridge that gap.”
Joe Williams, specialist cancer and lead homecare pharmacist at the Christie Hospital in Manchester, and chair of the British Oncology Pharmacy Association, feels the system works well in his area, with sharing and monitoring of KPIs at monthly regional meetings. But he points out that the process of homecare prescription management does put pressure on pharmacy departments.
“The paperwork around homecare is substantial. We have to print out prescriptions from our SACT [systemic anti-cancer therapy] prescribing system, get them signed, email them to the companies and then physically mail them too. This is something which needs urgent digital development,” he says.
The NHS Benchmarking Network data show that, within pharmacy homecare teams, 52% of roles are admin or ‘other’, with 23% being pharmacist roles and 25% being pharmacy technician roles.
Removing some of the administration may mean existing staff can cope with a greater number of patients, but that is unlikely to be enough to cope with the rising numbers of patients signing up to homecare. More investment will be needed, including in training staff, suggests Allen.
Alternative models
Clare Jacklin, chief executive of the National Rheumatoid Arthritis Society, questions whether some sort of change to the delivery system is needed to cope with the increase in demand. “Homecare services need to scale up to meet the demands of this bigger volume,” she says, “or find other ways of meeting the increasing demand.”
Allen suggests that some medicines currently delivered through homecare services could be switched to other delivery routes; for example, the newer oral agents used in services such as gastroenterology or rheumatology. Developing different supply mechanisms with appropriate specialist oversight and monitoring could open up more capacity in homecare for more complex drugs. However, he points out that some of these medicines are currently only available to purchase as part of a homecare bundle.
Ross Maclagan, distribution and supply chain policy manager at the Association of the British Pharmaceutical Industry, suggests one solution might be to have less frequent deliveries for patients who are stable, allowing capacity to be directed towards less stable patients who may need more frequent changes in medication.
The demand for homecare services is likely to continue to increase in the future as more innovative medicines are introduced. For example, if new disease-modifying drug infusions for Alzheimer’s disease, such as lecanemab — currently being considered by the MHRA under its accelerated ‘Innovative Licensing and Access Pathway’ — become available to even a fraction of the people with dementia in the UK, it would risk overwhelming hospital capacity to deliver these. A homecare system that functions well will be vital.
- 1Gregory A. Regulator to review safety concerns over medicines courier used by NHS. The Guardian. 2023. https://www.theguardian.com/society/2023/apr/21/regulator-to-review-safety-concerns-over-medicines-courier-sciensus-nhs (accessed 8 November 2023)
- 2Gregory A. Seriously ill children put at risk by firm’s failure to deliver NHS medication. The Guardian. 2023. https://www.theguardian.com/society/2023/may/09/seriously-ill-children-put-at-risk-by-firms-failure-to-deliver-nhs-medication-sciensus (accessed 8 November 2023)
- 3Chibelushi W. Sciensus: Chronically ill patients go without vital drugs amid delays by NHS-contracted firm. ITVX. 2023. https://www.itv.com/news/2023-04-21/chronically-ill-patients-go-without-drugs-amid-delays-by-nhs-contracted-firm (accessed 8 November 2023)
- 4Public Services Committee. Homecare medicines services inquiry. UK Parliament. 2023. https://committees.parliament.uk/work/7739/homecare-medicines-services/ (accessed 8 November 2023)
- 5Public Services Committee: Corrected oral evidence: Homecare medicines services. House of Lords. 2023. https://committees.parliament.uk/oralevidence/13633/html/ (accessed 8 November 2023)
- 6Public Services Committee: Corrected oral evidence: Homecare medicines services. House of Lords. 2023. https://committees.parliament.uk/oralevidence/13323/html/ (accessed 8 November 2023)
- 7Public Services Committee: Corrected oral evidence: Homecare medicines services. House of Lords. 2023. https://committees.parliament.uk/oralevidence/13411/html/ (accessed 8 November 2023)
- 8Homecare Services Professional Standards. Royal Pharmaceutical Society. https://www.rpharms.com/recognition/setting-professional-standards/homecare-services-professional-standards (accessed 8 November 2023)
- 9Homecare Handbook Appendices. Royal Pharmaceutical Society. https://www.rpharms.com/recognition/setting-professional-standards/homecare-services-professional-standards/homecare-handbook-appendices (accessed 8 November 2023)
- 10National Homecare Medicines Committee. National Homecare Medicines Committee (NHMC) Proposal for the funding of Pharmacy Homecare Teams. Specialist Pharmacy Service. 2021. https://www.sps.nhs.uk/wp-content/uploads/2018/05/NHMC-Proposal-for-the-Funding-of-Pharmacy-Homecare-Teams-FINAL-March-2021-v2.0.pdf (accessed 8 November 2023)
1 comment
You must be logged in to post a comment.



We must also consider the environmental impact of homecare services. Medicine deliveries to individual patients by road across the UK from a centralised company does not appear sustainable.