


Connect Images / Alamy Stock Photos
Nearly 200 community pharmacies participated in NHS England’s independent prescribing (IP) pathfinder project in 2025, delivering a range of services from minor ailments to long-term conditions, such as cardiovascular disease and respiratory disease, as well as support with lipid management, deprescribing and menopause.
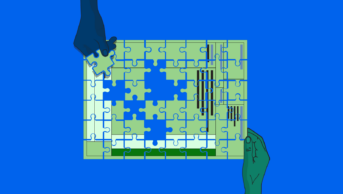
Figure: Where the pathfinder sites are and what they are exploring
The pathfinder programme was set up by NHS England in 2024 to test how community pharmacist prescribing could work, what hurdles would need to be overcome and how it could be incorporated into nationally-commissioned NHS services.
Findings of an evaluation of the project, conducted by the University of Manchester and published on 8 January 2025, showed that many participating pharmacist prescribers reported increased job satisfaction and the ability to use their clinical skills to much better effect.
As of 31 July 2025, 197 sites across 40 integrated care boards (ICBs) had registered to take part in the pathfinder programme. According to the data from NHS England cited in the evaluation report, pathfinder sites delivered more than 33,000 consultations, with 97% concluding without the need for patients to be seen by anyone else.
However, figures from NHS England’s most recent ‘Community pharmacy workforce survey’, published in July 2025, show that the majority (an estimated 93%) of independent prescribing (IP) pharmacists in community pharmacies in England are not using their qualification in community pharmacy, despite their numbers continuing to grow.
In October 2025, responses from The Pharmaceutical Journal’s latest salary survey also revealed that just under half of pharmacists across the whole profession who hold an IP qualification use it daily (48%, n=122), although this dropped to three in ten (30%, [n=3]) community pharmacist respondents who held an IP qualification.
The University of Manchester’s evaluation recorded pathfinder participants’ views that prescribing should not be seen as an isolated service.
“This was because IP was not just about prescribing but also about providing holistic patient care, which requires broader clinical consideration and collaboration between IP pharmacists and the GP practice,” it said.
Access to pathology was found to be one of the major challenges in implementing long-term condition models and novel services
Evaluation of the pathfinder project by the University of Manchester
The findings suggested that the way community prescribing could be implemented was “was primarily dependent on whether they targeted acute or long-term conditions”.
The report concluded that both approaches required good relationships with other local partners, particularly GPs and other pharmacies, supported by the local ICB.
In particular, the management of long-term conditions in community pharmacy presented the pathfinder sites with a series of challenges to overcome: access to pathology; digital infrastructure; clinical supervision; workforce; clinical governance; and funding — all of which are required if IP pharmacists are to offer holistic patient care.
Pathology
“Access to pathology was found to be one of the major challenges in implementing long-term condition models and novel services, which require blood test results”, the evaluation found.
Pharmacists struggled to order blood tests and check results, and were not usually connected into the necessary systems to do so. The evaluation recommended that NHS England give community pharmacies “access/ infrastructure to diagnostics, such as phlebotomy, recognising it as a key element of future clinical services”.
Digital infrastructure
Pharmacies taking part in the pathfinder sites were given access to NHS electronic prescribing solution (EPS) ‘CLEO’.
While CLEO allowed sites to issue electronic prescriptions, sites still experienced issues with connecting to patient records and other clinical systems such as secondary care records. Most pharmacists interviewed for the evaluation “expressed frustration over having to use multiple platforms, which led to duplicated effort, manual data entry and the potential for crucial information to be missed”, as well as extending the consultation time.
Interviewees underscored the need for an integrated IT system with full read/write access to patient records
Evaluation of the pathfinder project by the University of Manchester
Meanwhile, the GP connect system offered limited read/write access to patients’ full medical histories, which pharmacists said “impacted their ability to prescribe safely”, the evaluation said.
“Interviewees underscored the need for an integrated IT system with full read/write access to patient records. Such a system was seen as essential to support seamless patient care, enable true collaboration, and ensure accountability through a clear audit trail.”
Clinical supervision
The evaluation report found that most pathfinder sites established formal clinical supervision, often provided by a GP, through regular one-to-one sessions, which helped to build prescriber confidence and GP trust. It also highlighted the value of informal support networks (peer support) for sharing learning and fostering collaboration.
However, the report noted that sites participating in the pathfinder project “were usually high-performing pharmacies, often with strong pre-existing relationships with GP practices and a track record in delivering clinical services”.
“This may not represent typical community pharmacies in England, many of which may lack the same resources and readiness,” it said.
In particular, GP buy-in was identified as “essential” for the management of long-term conditions, the report said, including “for ensuring the safe transfer of care and providing a more integrated service for patients”.
Where there was no existing relationship, the ICB facilitated it, including through dedicated staff roles. The report also recommended that, in a future service, ICBs should fund protected time for prescribing pharmacists to build relationships with local GPs.
Nevertheless, issues around GP capacity remain unresolved. Although funding for GPs was available, the report deemed the amount as inadequate, with the current shortage of GPs making it challenging to absorb this additional demand on their time.
One programme manager quoted in the evaluation report said this made getting GP buy-in difficult because pharmacies were “trying to sell [pathfinders] on the concept that it would take work away from [GPs]”.
Funding
A total of £12m in funding was allocated to the programme, some of which was available to participating pharmacies via a one-time core set-up fee of £1,500 per pharmacy premises to cover IT support and participation in evaluation activities.
In some cases, an additional set-up fee was made available (if applicable), depending on the service model as agreed with the ICB . Sessional payments for IP delivery were offered, whereby independent prescribing pharmacists were expected to deliver up to six sessions per week, up to a maximum of 24 sessions per month, designed to be flexible and cover all necessary activities, including patient consultation, documentation and meetings with supervisors.
However, the evaluation said “a common view was that pathfinder participation could cost more than the funding provided”.
Moreover, pharmacies needed to be financially sustainable to continue offering IP services. Many independent pharmacy owners worked additional unpaid hours, “driven by the motivation to demonstrate what pharmacy could contribute”, while some sites that had dropped out of the pathfinder programme cited “a lack of capacity and resources”, the report concluded.
The sector’s view
Malcolm Harrison, chief executive of the Company Chemists’ Association, said: “Changes to pharmacy supervision and the rollout of independent prescribing present a significant opportunity to increase clinical capacity in primary care through community pharmacy, improving both patient access and outcomes.
“A key starting point should be to ensure prescribers can use their full skillset within the Pharmacy First service,” he suggested.
Skill‑mix change must be funded and planned, not left to goodwill
Pharmacists’ Defence Association
“The evaluation rightly recognises the need for integrated technology, access to clinical records and diagnostics, standardised governance frameworks and sustainable funding. These are essential to delivering consistent standards of care nationwide and maintaining the confidence of patients and other healthcare professionals. This standardisation across the country will be critical to the successful transition to a prescribing-enabled workforce,” Harrison added.
But the Pharmacists’ Defence Association (PDA) said supervision reform “must genuinely release pharmacists for clinical care”.
In a statement made to The Pharmaceutical Journal, the PDA said: “Pathfinder sites show that IP consultations routinely run 15–30 minutes or more, requiring full history‑taking, clinical decision‑making, documentation and follow‑up for long‑term conditions. Expecting pharmacists to deliver this while simultaneously accuracy‑checking, managing workflow and handling front‑of‑house demands fragments time and raises stress.
“Supervision reform should therefore actually free pharmacists from routine dispensing so they can provide safe, sustainable clinical care.”
The PDA stressed the need for role clarity: “Skill‑mix change must be funded and planned, not left to goodwill.”
Responding to the report, a spokesperson for NHS England told The Pharmaceutical Journal that it “will use these findings to help us develop future clinical services within pharmacy and as we deliver on the ten-year health plan, which [aims] to improve patient access to services in the community, and pharmacies will have an integral role in that work”.
1 comment
You must be logged in to post a comment.


One reason why pharmacists may not be able to deliver satisfactory long-term health care is that the patients themselves and their medical conditions change over time, and these changes need to be recognized and monitored.
In my own case, for treatment of my moderately high blood pressure, which is increasing with age, I would be happy to be treated by my pharmacist if there was a robust agreement in place for me to be sent to see my doc if there was a significant change in my health, perhaps requiring a change in treatment, or even a different treatment.