


Phanie / Alamy
In this article you will learn:
- When medicines may be considered to manage aggressive behaviour
- The medicines and formulations that may be used, and their risks and benefits
- How to assess patients following sedation to avoid inappropriate use
Patients can present with challenging and sometimes violent behaviour in a range of healthcare settings. Challenging behaviour is defined as any non-verbal, verbal or physical behaviour which makes it difficult to deliver good care safely. It can include grabbing, biting, punching, or self-injury[1]
. The patient may not be aware of their actions. According to the NHS Business Services Authority[2]
, there were a total of 68,683 assaults against NHS staff in 2013–2014, with 53,484 incidents involving medical factors where the perpetrator did not know what they were doing.
Some patients require restraint, and most incidents requiring a patient’s restraint occur in acute medical wards[1]
. Around 30% of all patients admitted to an acute ward have a co-morbid mental health condition, rising to 45% in older people, compared with only 5% of patients seen in accident and emergency departments. The most common mental health conditions seen in acute hospitals are depression, delirium, dementia, adjustment disorder (i.e. inability to cope with a stressful life event) and alcohol-related presentations.
This article focuses on the use of medicines for patients with challenging behaviour. However, medicines should never be the first option considered, and preventing this behaviour occurring is as important as management.
Initial presentation
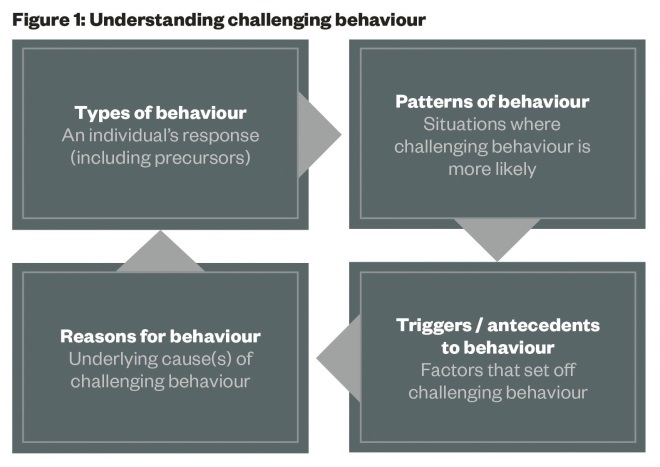
Before an effective plan can be put in place to manage challenging behaviour, it is crucial to understand why the patient’s behaviour is disturbed (see ‘Understanding challenging behaviour’). Patients are often in an unfamiliar setting, are not feeling well and may be frightened.
Causes include but are not limited to:
- Physical – pain, delirium, other medicines (either being ineffective or actively causing problems), epilepsy (before and after seizures);
- Cognitive – communication difficulties (any cause), learning disability, autism, dementia;
- Substance misuse – illicit substance or alcohol misuse (withdrawal symptoms or intoxication);
- Psychological or emotional – stress, anxiety, fear.
Source: NHS Protect. Meeting needs and reducing distress: Guidance on the prevention and management of clinically related challenging behaviour in NHS settings
If a person is aggressive or violent, short-term interventions include de-escalation (techniques to defuse the situation), physical restraint and moving the patient to an alternative setting (quieter, less stimulation or more restrictive). Good communication should be part of the overarching strategy to de-escalate the situation, calm the patient down and reduce distress and anxiety[1]
.
The National Institute for Health and Care Excellence (NICE) recommends all health organisations give staff training in de-escalation, which includes:
- recognising the early signs of agitation, irritation, anger and aggression;
- understanding the likely causes of aggression or violence;
- techniques for distraction and calming, and ways to encourage relaxation;
- recognising the importance of personal space;
- responding to a patient’s anger in an appropriate, measured and reasonable way to avoid provocation.
Ultimately, these interventions may involve the psychiatric liaison team[3]
or the police. The use of medicines could potentially be considered alongside any of these options.
NICE recommends that a formal external post-incident review takes place no later than 72 hours after the incident, and should include staff from outside where the incident took place, such as from another ward. The information is recorded and included in the patient’s notes[4]
.
Pharmacological management
Medicines can be a useful management option, particularly if the behaviour is specifically of a psychiatric origin (e.g. psychosis or mania) or where the behaviour is putting either the patient or others at a significant immediate risk
[1]
,
[5]
.
Medicines should only be used when the risks of not doing so are greater than the inherent risks of introducing a medicine into an already stressful situation. Healthcare teams need to consider:
- the risks to either the patient or to other people;
- the consequences of potentially escalating violence;
- the risks of potential adverse effects of medicines.
In principle, an oral medicine should always be offered and used where possible. Parenteral options should only be considered when oral administration is not feasible[4]
. NICE states that patients, or their carers, should have the opportunity to make informed decisions about their care. However, if someone does not have the capacity to make decisions, the safeguards outlined in the Mental Capacity Act 2005 should be followed.
Whichever route is chosen, the medicine needs to have a very rapid onset of action, with an effect lasting for just a few hours. NICE uses the term ‘rapid tranquillisation’ to define using medicines parenterally to reduce the risk of harm and minimise agitation and violence[4]
.
A small range of medicines are available for oral or parenteral, usually intramuscular, administration. The most commonly recommended options are the benzodiazepine lorazepam and the typical antipsychotic haloperidol, and both have clear evidence to demonstrate efficacy[4],[6],[7],[8]
(see ‘Medicines used to manage patient aggression’).
Benzodiazepines can theoretically cause significant sedation leading to respiratory depression, which can be reversed with intravenous flumazenil.
Lorazepam is short-acting with no active metabolites, and respiratory depression is extremely unlikely with prescribed doses. Lorazepam is therefore a safer first-line option than other, longer-acting, benzodiazepines, such as diazepam. Diazepam should not be used intramuscularly for rapid tranquillisation[9]
, and the response with intravenous use is less predictable, and also increases the patient’s risk of respiratory depression.
Haloperidol is not recommended as first-line monotherapy. This is because it can increase the QT interval, which could lead to cardiac arrhythmias or torsades de pointes, and can also cause extrapyramidal side effects. Both of these adverse effects are dose-related, and the latter can be treated with anticholinergic medicines, such as procyclidine. It can be given orally or intramuscularly, and can be used concurrently with lorazepam
[5]
. Haloperidol is no longer licensed for intravenous use[10]
.
| Medicines used to manage patient aggression | |||||
|---|---|---|---|---|---|
| Medicine | Route | Onset of effect | Time to peak effect | Duration of effect | Reversing agent |
Aripiprazole | Intramuscular | 30–45 minutes | 1–3 hours | 18–24 hours | None |
Diazepam | Intravenous | 5–10 seconds | <1 minute | 12–24 hours | Flumazenil |
Haloperidol | Oral | 1–2 hours | 2–6 hours | 18–24 hours | None |
Haloperidol | Intramuscular | 15–30 minutes | 20 minutes | 18–24 hours | None |
Lorazepam | Oral | 20–30 minutes | 2 hours | 6–8 hours | Flumazenil |
Lorazepam | Intramuscular | 15–30 minutes | 60–90 minutes | 6–8 hours | Flumazenil |
Olanzapine | Oral | ≈ 2 hours | 5–8 hours | 24 hours | None |
Olanzapine | Intramuscular | 15–30 minutes | 15–45 minutes | 24 hours | None |
Promethazine | Intramuscular | 30–60 minutes | 1–2 hours | 10 hours (2–8 hours) | None |
Olanzapine
is
an atypical antipsychotic. It should not be given by intramuscular injection concurrently with intramuscular lorazepam because of the risk of respiratory depression and bradycardia when used together (although they can be given
together orally). At least a two-hour gap should be allowed between doses[11]
.
Promethazine, given by intramuscular injection, is a potential alternative when intramuscular lorazepam is not available. It is not licensed for this indication, but its efficacy has been demonstrated both as monotherapy and in conjunction with haloperidol[12]
. Promethazine has a slower onset of action than other options, such as intramuscular lorazepam, which can be problematic if the patient is being restrained. Oral promethazine is not recommended for this indication as it has a slow onset of action.
Aripiprazole, given by intramuscular injection, has a weaker evidence base for efficacy in rapid tranquillisation than other, more established medicines. It can be given with lorazepam, and together has a greater effect than aripiprazole as monotherapy[13]
.
Within psychiatric settings, where the reason for the acutely disturbed behaviour is often psychotic in nature, patients may benefit from being given an antipsychotic if one has not already been prescribed[14]
, particularly if the use of a benzodiazepine alone has been insufficient[15]
.
Long-term management
Repeated patterns of disturbed behaviour can be problematic in a number of chronic scenarios such as in dementia, or in patients with learning disabilities or autism. If repeated incidents of violent or disturbed behaviour occur it is crucial not to just repeat the same management plan. The overall picture should be reviewed, and the target symptoms, causes or contributing factors should be identified and addressed; the focus should be on preventing further events.
Plans should also be put in place to address medium-term goals. These may or may not involve the use of medicines. In addition to a thorough review of the presentation and diagnosis related to the behaviour, any regularly prescribed medicines should be optimised, and any contributing or aggravating factors should be excluded (as far as possible). Without a thorough review of the situation, medicines used acutely to control the behaviour may cause more harm than good.
For example, in patients with dementia, clinicians should ensure the main treatment of the dementia itself (usually acetylcholinesterase inhibitors) is optimised before adding in regular or as required oral antipsychotics for the management of behavioural symptoms. Similarly, causal or precipitating situations around an individual patients’ disturbed behaviour should be reviewed, such as routine patterns and arrangements around washing and dressing or eating, rather than making medicines the tool that is automatically used to manage predictable episodes of disturbed behaviour[16],[17]
.
Medicines should only be used to control or subdue disturbed or violent behaviour when other therapeutic options have been tried and have failed. This applies to all settings. Pharmacists should regularly review the ongoing use of prescriptions for hypnotics and other sedating medicines, such as antipsychotics or sedating analgesics, to determine if they are clinically appropriate.
If treatment is used to reduce the risk of violence and aggression, NICE recommends a multidisciplinary team reviews the pharmacological strategy at least once a week, or more frequently if the problem is getting worse or more restrictive treatments are being planned or used. This review should be recorded, and include:
- Clarification of target symptoms;
- Likely timescale for response;
- Total daily dose of medicines, including as required (both prescribed and administered);
- Missed doses and the reason doses were missed;
- Therapeutic response;
- Any adverse effects.
Rapid tranquillisation should be reviewed at least once a day by a senior doctor.
Further reading
The NHS Protect guidance[1]
gives extensive guidance around the management of aggressive and violent behaviour in any healthcare setting, with particular reference to accident and emergency departments and acute hospitals. It mentions the role of medicines, but as a non-clinical document, it does not give detailed advice.
Detailed guidance on the acute management of patients with challenging or violent behaviour driven by a mental health disorder (regardless of the setting that they are in) and the use of rapid tranquillisation is available from the National Institute for Health and Care Excellence
[4]
. The guidance applies to adults, children and young people who have a mental health problem and whose behaviour is violent or aggressive in all settings.
The role of medicines in the long-term management of aggressive and violent or antisocial behaviour is beyond the remit of this article. Further reading is available from the Royal College of Psychiatrists
[18]
.
Additional guidance on this and in specific patient groups, such as in patients with learning disabilities, is also available from the Maudsley prescribing guidelines[19]
and the Royal College of Psychiatrists[20]
.
Caroline Parker FFRP
S, FRPharmS, FCMHP is a c
onsultant pharmacist in adult mental health at
Central and North West London
NHS Foundation Trust.
References
[1] NHS Protect. Meeting needs and reducing distress: Guidance on the prevention and management of clinically related challenging behaviour in NHS settings. Available from: www.nhsprotect.nhs.uk/reducingdistress.
[2] NHS Business Services Authority. Number of reported physical assaults on NHS staff in 2013/14. London: NHSBSA 2015.
[3] Royal College of Psychiatrists. Liaison psychiatry for every acute hospital: Integrated mental and physical healthcare. CR183. London: RCPsych 2013.
[4] National Institute for Health and Care Excellence. Violence and aggression: short-term management in mental health, health and community settings. London: NICE 2015.
[5] TREC Collaborative Group. Rapid tranquillisation for agitated patients in psychiatric rooms: a randomised trial of midazolam versus haloperidol plus promethazine. BMJ 2003;327(7417):708–711.
[6] Innes J & Sethi F. Current rapid tranquillisation documents in the UK: a review of the drugs recommended, their routes of administration and clinical parameters influencing their use. J Psychiatric Intensive Care 2012. doi:10.1017/S174264641200026X.
[7] Huf G, Coutinho ESF, Adams CE et al. Rapid tranquillisation in psychiatric emergency settings in Brazil: pragmatic randomised controlled trial of intramuscular haloperidol versus intramuscular haloperidol plus promethazine. BMJ 2007;335(7625):869–875.
[8] Raveendran NS, Tharyan P, Alexander J et al. Rapid tranquillisation in psychiatric emergency settings in India: pragmatic randomised controlled trial of intramuscular olanzapine versus intramuscular haloperidol plus promethazine. BMJ 2007;335(7625): 865–872.
[9] Actavis UK Ltd. Diazemuls, Diazepam Actavis 5mg/ml Emulsion for Injection. Summary of Product Characteristics. Last updated on eMC 18 March 2015.
[10] Amdipharm Mercury Company. Haloperidol Injection BP 5mg/ml. Summary of Product Characteristics. Last updated on eMC 14 February 2014.
[11] Eli Lilly and Company Limited. Zyprexa Powder for Solution for Injection. Summary of Product Characteristics. Last updated on eMC 4 June 2014.
[12] National Institute for Health and Care Excellence. Rapid tranquillisation in mental health settings: promethazine hydrochloride. London: NICE 2014.
[13] Otsuka Pharmaceuticals (UK) Ltd. Abilify 7.5 mg/ml solution for injection (intramuscular). Summary of Product Characteristics. Last updated on eMC 7 November 2014.
[14] Agid O, Kapur S, Arenovich T et al. Delayed-onset hypothesis of antipsychotic action: a hypothesis tested and rejected. Arch Gen Psych 2003;60(12):1228–1235.
[15] Gillies D, Sampson S, Beck A et al. Benzodiazepines for psychosis-induced aggression or agitation. Cochrane Datab Syst Rev 2013 30;4:CD003079. doi:10.1002/14651858.CD003079.pub3.
[16] Banerjee S. The use of antipsychotic medication for people with dementia: time for action. A report for the Minister of State for Care Services. London: RCPsych 2009.
[17] The King’s Fund. Polypharmacy and medicines optimisation. Making it safe and sound. London: The King’s Fund 2013.
[18] Beer D & Khwaja M, eds. Prevention and management of violence: guidance for mental healthcare professionals. CR177. London: RCPsych 2013.
[19] Taylor D, Paton C & Kapuar S. The Maudsley Prescribing Guidelines, 11th ed. London: Wiley-Blackwell 2012.
[20] Royal College of Psychiatrists. The evidence base for the management of imminent violence in learning disability settings. Occasional Paper OP57. London: RCPsych 2005.


