

Key points:
- Fibromyalgia is a common and high-impact disorder;
- Fibromyalgia is characterised by chronic pain, poor sleep, fatigue, cognitive dysfunction and emotional distress;
- Fibromyalgia management encompasses education, exercise, psychological strategies and use of drugs;
- Drug management in fibromyalgia targets pain modulatory mechanisms;
- Serotonin-noradrenaline reuptake inhibitors, tricyclic antidepressants and gabapentinoids have moderate efficacy in fibromyalgia;
- Pure opioids have little role in fibromyalgia;
- There is a need for new drugs targeting the fibromyalgia mechanism.
Introduction
Fibromyalgia is a common condition characterised by abnormal central nervous system sensitivity to external stimuli. It affects between 2 and 8% of the total population, with a strong female predominance[1],[2]
. The most recognisable clinical feature associated with fibromyalgia is widespread pain and tenderness throughout multiple regions of the body, in the absence of pathology at the sites of pain. Patients may also experience a wide variety of other symptoms including fatigue and sleep disturbance, cognitive changes such as poor concentration and memory, and amplified sensory systems leading to an intolerance of loud noise, bright lights and strong odours[3]
,[4]
. Medication side effects are commonly exacerbated in this patient population and many drugs are poorly tolerated. Fibromyalgia is associated with several related medical conditions including irritable bowel syndrome, temporomandibular joint dysfunction, tension headaches, chronic fatigue syndrome and restless leg syndrome[1]
.
The pathophysiology of fibromyalgia is complex, although understanding has increased substantially in recent years. The net effect of multiple factors leads to a sensitisation of central pain and sensory processing centres such that patients become overly sensitive to external stimuli. Functional imaging studies have shown amplified responses in sensory regions of the brain when mechanical or painful stimuli are administered[5]
,[6]
. There is also evidence of enhanced connections between brain centres that process pain and sensory input, such as the insular cortex, and parts of the brain associated with concentration and working memory, such as the frontoparietal executive attention network[5]
. This may provide some explanation for the cognitive symptoms many patients experience. Several abnormalities of neurotransmitters have also been identified in fibromyalgia patients, and relate to modulation of descending sensory inhibitory pathways from the brain to the spinal cord. These are discussed in relation to specific pharmacological interventions in later sections.
Fibromyalgia has a strong genetic predisposition — twin studies suggest the contribution is as high as 50%[7]
. In genetically susceptible individuals, symptoms tend to be triggered by a stressful event such as physical illness, trauma or psychological distress[4]
. Symptoms of fibromyalgia wax and wane over time, and tend to be exacerbated by fluctuations in psychological or physical stress.
Diagnosis of fibromyalgia is based on the identification of characteristic clinical features. Validated diagnostic criteria are available and require the presence of widespread pain in conjunction with high levels of some of the above mentioned associated symptoms (see Figure 1)[3]
.
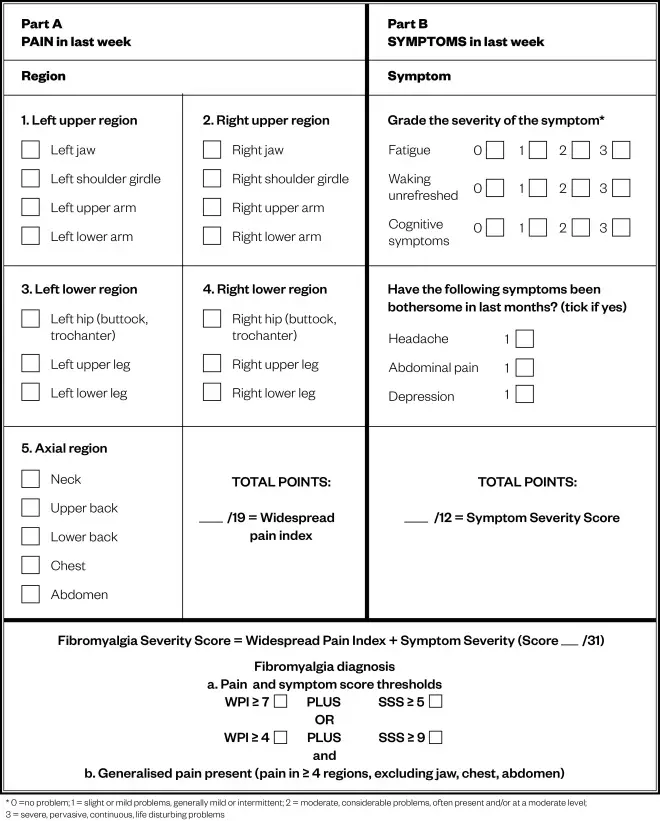
Figure 1: 2016 American College of Rheumatology diagnostic criteria for fibromyalgia
Source: Reproduced with permission from the American College of Rheumatology[3]
Diagnosis of fibromyalgia is based on the identification of characteristic clinical features. Validated diagnostic criteria are available and require the presence of widespread pain in conjunction with high levels of associated symptoms
Healthcare professionals should obtain a careful history from the patient and undertake a detailed clinical examination to identify other problems that may cause widespread pain, such as inflammatory arthritis and mechanical musculoskeletal problems, or hormonal disorders such as those associated with menopause. However, it is well recognised that fibromyalgia commonly occurs concurrently in patients who have other comorbidities, particularly those that are long-lasting, stressful or painful, and should not be considered a diagnosis of exclusion[3]
,[8]
,[9]
. Blood screening tests are usually performed to exclude any common biochemical or hormonal abnormalities, such as iron or vitamin D deficiency or thyroid function abnormalities, which may mimic or exacerbate fibromyalgia symptoms. Inflammatory markers are generally normal. This article focuses on the options for pharmacological management of fibromyalgia.
Sources and selection criteria
The articles discussed here were identified from the authors’ own databases and were supplemented with searches on PubMed/MEDLINE and online journals. The following keywords were used in various combinations: “fibromyalgia, management, medication, drugs, guidelines”. The bibliography of relevant identified papers was scanned and information from abstracts and online sources was included as deemed relevant.
Management of fibromyalgia
Fibromyalgia can have a substantial impact on both a patient’s mental and physical health. Low work participation, high rates of financial dependency and poor quality of life are all well described in this population[10]
,[11]
. Treatment of fibromyalgia is aimed at modulating central pain pathways to reduce sensitivity, which can be obtained via a range of treatment modalities. The most recently published guidelines are the 2016 European League Against Rheumatism (EULAR) fibromyalgia management guidelines, and the 2012 Canadian fibromyalgia diagnosis and management guidelines, and these are referred to and discussed in this article[12]
,[13]
.
The mainstay of treatment is non-pharmacological. Evidence-based treatment strategies with the highest efficacy include education in relation to the nature of the condition, graded exercise programmes, and psychological-based interventions. These may range from cognitive-based stress management therapy with a pain management psychologist to yoga, tai-chi or simple meditation strategies. These non-pharmacological interventions are recommended by EULAR as first-line treatments[12]
. More than 30 trials involving more than 2,000 fibromyalgia patients have been performed evaluating various forms of exercise, and a further 2,000 patients have been involved in trials of cognitive based therapy (CBT)[12]
,[14]
. Both aerobic and strengthening exercises have been shown to significantly reduce pain and increase function, with CBT also proving effective, albeit with lower quality evidence[14]
,[15]
. The EULAR guidelines provide a thorough review of the evidence to support the various non-pharmacological strategies available[12]
.
However, many patients require the addition of pharmacological therapy for the management of their symptoms. It should be noted that medication is unlikely to be of benefit in isolation in the absence of the above-mentioned strategies.
Medications recommended for the treatment of fibromyalgia
Several medications have shown some efficacy in the management of fibromyalgia. Availability and condition-specific approval of medications vary across countries (see Table 1). There are currently no medications with fibromyalgia-specific approval under the European Medicines Agency, although many of the discussed agents are approved for other conditions. Many patients will respond to some degree to one or more of the discussed medications, although each individual medication is only effective in a minority of patients. Patients may need to trial several options before finding one that is both tolerable and helpful.
| Table 1: Availability and approval of recommended medications for fibromyalgia [13] ,[16] ,[17] ,[18] | ||||||||
|---|---|---|---|---|---|---|---|---|
| *France, Portugal, Finland, Estonia, Austria, Luxembourg, Poland, Turkey, Bulgaria and Russia. | ||||||||
| Europe | United States | Australia | Canada | |||||
| Drug | Available | Approved for fibromyalgia | Available | Approved for fibromyalgia | Available | Approved for fibromyalgia | Available | Approved for fibromyalgia |
| Amitriptyline | Yes | No | Yes | No | Yes | No | Yes | No |
| Cyclobenzaprine | No | No | Yes | No | No | No | Yes | No |
| Duloxetine | Yes | No | Yes | Yes | Yes | No | Yes | Yes |
| Milnacipran | Some countries only* | No | Yes | Yes | Yes | Yes | No | No |
| Pregabalin | Yes | No | Yes | Yes | Yes | No | Yes | Yes |
| Tramadol | Yes | No | Yes | No | Yes | No | Yes | No |
Serotonin and noradrenergic reuptake inhibitors (SNRIs)
Serotonin and noradrenaline are neurotransmitters involved in pain-processing pathways via their action on descending inhibitory pathways in the brain and spinal cord, with the net effect of reducing sensory input from the periphery[19]
. Both neurotransmitters have an array of other functions including roles in regulation of mood and emotion, with noradrenaline also involved in regulation of attention and memory[19]
.
The cerebrospinal fluid (CSF) of patients with fibromyalgia has been shown to have lower levels of biogenic amines, the metabolites of noradrenaline and serotonin, suggesting a deficiency of these neurotransmitters[20]
. Studies using murine models have shown that modulation of noradrenaline and serotonin in unison provides more effective analgesic effects than modulation of serotonin alone[21]
. However, there is no direct comparative study between SNRIs and selective serotonin reuptake inhibitors (SSRIs) in fibromyalgia. Two SNRI medications, duloxetine and milnacipran, are recommended for the treatment of fibromyalgia. Milnacipran is not approved by the European Medicines Agency, but it is approved in several European countries for indications other than fibromyalgia, such as depression (see Table 1).
Duloxetine is an SNRI originally marketed for the treatment of depression, but several studies have since evaluated its benefit in fibromyalgia[22]
,[23]
,[24]
. A meta-analysis of six randomised trials of duloxetine compared with placebo in more than 2,000 patients with fibromyalgia showed a significant improvement in a pain reduction at weeks 12 and 28. Overall, the number needed to treat was eight[25]
.
Doses can range from 30 to 120mg daily, however, many patients with fibromyalgia cannot tolerate doses above 60mg. Common side effects include headache, palpitations, nausea and flushing. Some patients find that duloxetine causes drowsiness and should take it before bed, while a smaller number of patients find it stimulating, and thus benefit more from taking it in early in the day.
Milnacipran is another SNRI recommended for the management of fibromyalgia. Trial data suggest that milnacipran improved quality of life and patient reported pain in around 15% of participants above that of placebo[26]
. The usual marketed dose of milnacipran is 50mg twice daily. However, many patients only tolerate much smaller doses, such as 25mg once or twice daily. Patients should be initiated on a dose of 25mg daily and then titrated upwards by 25mg daily at a minimum of every few days. Milnacipran has a similar side effect profile to duloxetine, but has stronger noradrenergic qualities than duloxetine and for this reason may be more stimulating[27]
.
Patients with prominent fatigue symptoms may benefit from SNRIs, in particular milnacipran, but they may be less appropriate for those patients with significant insomnia. Concurrent depressive or anxiety symptoms may be another reason for the preference of these agents in individual patients[28]
.
Duloxetine is metabolised via the cytochrome (CY) P450 2D6 pathway, a system which metabolises around 25% of clinically used drugs, and there is therefore a high risk of drug interactions[29]
. Variations in metabolism of duloxetine can occur due to polymorphisms of the 2D6 gene. By comparison, milnacipran is not metabolised via the CYP450 pathway and, as such, drug interactions are much less likely[30]
.
SNRIs can be combined with pregabalin and simple analgesics, however, caution should be taken when combining SNRIs with tricyclic antidepressants or tramadol due to the potential risk of serotonin syndrome. Low doses in combination may be considered with careful patient education and monitoring. The symptoms of serotonin syndrome are variable and include cognitive changes such as agitation, autonomic symptoms (e.g. flushing and sweating), and neuromuscular symptoms (e.g. tremor)[31]
. The exact incidence of serotonin syndrome is unknown due to the lack of large studies and variations in diagnostic criteria, however, potent CYP450 2D6 inhibitors, increased age and higher doses increase the risk of this complication[31]
,[32]
. Most cases are mild and self limiting on drug cessation, however, rare severe cases can be life threatening. SNRIs are recommended in both the EULAR and Canadian Guidelines[12]
,[13]
.
Selective serotonin reuptake inhibitors (SSRIs)
As discussed above, modulation of serotonin alone is of less benefit than dual modulation of noradrenaline and serotonin together in the treatment of fibromyalgia. Several studies have evaluated the use of SSRIs in fibromyalgia with inconsistent results[33]
,[34]
,[35]
,[36]
. A meta-analysis of seven studies demonstrated some benefit when compared with placebo, although the quality of the study overall was low and the authors reported that there was no unbiased high-quality data to support the use of SSRIs in the management of fibromyalgia[37]
. The EULAR guidelines recommend against the use of SSRIs, while the Canadian guidelines suggest their use may be appropriate as an alternative to SNRIs[12]
,[13]
. Common side effects associated with SSRIs include nausea, sexual dysfunction, dry mouth, drowsiness and insomnia.
Gabapentinoids
Pregabalin was originally marketed as an antiepileptic but is now commonly used for pain management[38]
. It mediates its effects by binding to voltage gated calcium channels, reducing calcium influx at sensitised spinal cord neurons, thereby reducing the release of neuroactive molecules, including glutamate, substance P and noradrenaline, into the synapse[39]
. It has been shown that patients with fibromyalgia have increased levels of glutamate in their insula, an area of the brain involved in pain processing, and that pregabalin can reduce this, leading to an associated decreased level of perceived pain[40]
,[41]
. Several studies have evaluated its effectiveness in fibromyalgia, and a recent Cochrane Review reported pregabalin reduces pain with tolerable side effects in around 10% of patients above that of placebo[42]
.
The full dose of pregabalin given to patients can be as high as 300mg twice daily, but similarly with many other medications, patients with fibromyalgia are poorly tolerant of such doses. Pregabalin can be initiated at a dose of 25–75mg daily, with the additional 25–75mg every one to two weeks as tolerated. Common side effects associated with pregabalin include dizziness, somnolence and weight gain. If somnolence is prominent, patients may benefit from taking pregabalin only at night to enhance sleep and minimize daytime drowsiness. Drug interactions are uncommon and pregabalin can be safely added to SNRIs, tricyclic antidepressants (TCAs) and most analgesics. It may be best for patients with prominent pain and sleep disturbance, and is less effective for fatigue[28]
. Pregabalin is recommended in both the EULAR and Canadian guidelines[12]
,[13]
.
Gabapentin is another antiepileptic medication that is sometimes used to treat fibromyalgia. Gabapentin has a similar mechanism of action to pregabalin, and exerts its effects via modulating neuronal voltage gated calcium channels[39]
. It has a shorter half-life than pregabalin, and is usually given three or more times daily, which may make dose titration easier, however, this does increase pill burden. Gabapentin is cheaper than pregabalin and may be prescribed for this reason. A small randomised trial of 150 patients reported that patients taking 1200-2400mg of gabapentin were more likely to have a 30% reduction in their pain at week 12, with a response rate around 20% higher in the treatment group compared with placebo[43]
. However, a recent Cochrane Review concluded that there is currently insufficient evidence to recommend gabapentin for routine use in fibromyalgia treatment[44]
. The EULAR guidelines make no recommendation for or against gabapentin given limited data; however, the Canadian guidelines do not differentiate between pregabalin and gabapentin[12]
,[13]
.
Tricyclic antidepressants (TCAs)
Like SNRIs, TCAs mediate their effects via modulation of noradrenaline and serotonin, and were originally developed for the treatment of depression[45]
.
Amitriptyline is a TCA commonly prescribed for the management of fibromyalgia and short-term studies have shown clinical improvements in 15-20% of patients taking amitriptyline above that of placebo[46]
,[47]
,[48]
. Nortriptyline is an alternative option; however, fewer studies have examined the use of this agent.
Side effects from amitriptyline are common and include dry mouth, constipation, daytime drowsiness and mental clouding. Like pregabalin, patients may benefit from taking this medication in the evening to promote sleep and minimise daytime side effects. Typically, much smaller doses are used in fibromyalgia than in depression, with between 10mg and 25mg usually prescribed as an early evening dose, with doses above 50mg seldom being used for this indication. It can be co-prescribed with pregabalin, SSRIs and simple analgesics, and cautiously with SNRI medications as discussed above. It may be particularly helpful in patients in whom insomnia is a prominent clinical feature[28]
.
Cyclobenzaprine is a medication with a similar tricyclic structure to amitriptyline, but is not known to have antidepressant effects[49]
. It is available in the United States but not in the UK. A meta-analysis of the use of this medication in patients with fibromyalgia reported that it leads to symptomatic improvement in one in five patients[50]
. The side effects commonly associated with the use of cyclobenzaprine are similar to amitriptyline. Doses of 1–4mg at night have been shown to improve sleep[13]
. Both amitriptyline and cyclobenzaprine are recommended in the EULAR and Canadian guidelines[12]
,[13]
.
Tramadol
Tramadol is a weak opioid with mild serotonin-noradrenaline reuptake inhibition. A small study showed benefit of tramadol in combination with paracetamol in patients with fibromyalgia compared with placebo[51]
. In this study, patients were given 37.5mg of tramadol four times per day. While difficult to confirm, it is likely that the positive effects of tramadol in fibromyalgia are due to their SNRI activity as opposed to their opioid effect. As discussed in the next section, opioids are unlikely to be beneficial in fibromyalgia, with side effects likely to include drowsiness, dizziness and nausea. Tramadol is recommended in the EULAR fibromyalgia guidelines, however, in the Canadian guidelines, it is suggested that tramadol is reserved for those patients with significant symptoms not responding to the above-mentioned drug classes. It should be used with caution with SSRIs, SNRIs and TCAs and, as it is metabolised by CYP450 2D6 and 3A4 pathways, medications that are potent inhibitors of this pathway, such as paroxetine or fluoxetine, should be avoided[52]
.
Combination medications
It should be noted that in many of the discussed trials, medications were administered as a single agent in the absence of concurrent non-pharmacological management strategies, which is not consistent with the typical way these medications are used in clinical practice. Although there are limited data to support this approach, many patients who do not respond to a single agent receive combination therapy[53]
. A retrospective study reported that patients receiving either milnacipran or duloxetine in conjunction with pregabalin had improved pain scores compared with any of the three agents alone[54]
. A further study suggested that adding milnacipran to pregabalin resulted in higher response rates than pregabalin alone. However, not unexpectedly, there were also more side effects associated with dual therapy[55]
. Further studies are required to investigate the efficacy of combination therapy and drug interactions need careful consideration.
Medications that are not recommended in fibromyalgia
Anti-inflammatory medications
Non steroidal anti-inflammatory drugs (NSAIDs) and glucocorticoids act peripherally to reduce inflammation at the site of tissue damage. Given that the pain experienced by patients with fibromyalgia is not nociceptive, it is not surprising that these medications are not of particular benefit. Small studies have evaluated the use of both NSAIDs and low-to-moderate dose glucocorticoids in fibromyalgia and have found no benefit over placebo[47]
,[56]
,[57]
. Any concurrent inflammatory or mechanical musculoskeletal condition should be treated appropriately, which may include the use of these medications in some patients.
Opioids
Despite their common use, there is no evidence to suggest opioid medication is beneficial in fibromyalgia and, to the contrary, these medications may be associated with significant harm[58]
. There are no randomised trials available; however, longitudinal observational studies have suggested that patients with fibromyalgia taking opioid medications have worse outcomes than those patients not taking opioids in terms of pain, function and quality of life[59]
,[60]
.
There is evidence to suggest that patients with fibromyalgia have abnormal endogenous opioidergic activity. Patients with fibromyalgia have been shown to have reduced μ-opioid receptor binding in several central nervous system (CNS) centres that are involved in processing pain, including the amygdala, cingulate and nucleus accumbens[61]
. This reduced binding potential is associated with increased perceived pain. Furthermore, endogenous opioids have been shown to be elevated in the CSF of fibromyalgia patients[62]
. Together, these findings may be suggestive of a chronically activated endogenous opioid system leading to downregulation of opioid receptors[58]
. This explanation provides rationale for why fibromyalgia patients respond poorly to opioid medication. In line with this, it has been shown that patients with more fibromyalgia symptoms were likely to required significantly more opioid post joint replacement surgery than those patients with fewer fibromyalgia symptoms[63]
.
Beyond this, common opioid-related side effects such as drowsiness and mental clouding are likely to exacerbate symptoms of fibromyalgia. Enteral side effects of opioids may worsen irritable bowel syndrome which is commonly associated with fibromyalgia. A further concern is that of opioid hyperalgesia, which can occur with prolonged opioid use and causes a paradoxical increase in pain sensitivity[64]
. This phenomenon may be related to sensitisation of pro-nociceptive pathways secondary to opioid induced toll like receptor 4 (TLR4) activation in glial cells. TLR4 activation leads to the release of neuroexcitatory and proinflammatory products[65]
. Opioids, excluding tramadol, are not recommended by any current guidelines for the management of fibromyalgia.
Medications requiring more study to assess efficacy in fibromyalgia
Low dose naltrexone
Interestingly, small studies have evaluated the use of low dose naltrexone, an opioid antagonist, in fibromyalgia on the basis that fibromyalgia patients may have a chronically activated endogenous opioid system. It is likely that low doses of naltrexone exert an analgesic effect via antagonism of TLR4 as opposed to the opioid receptor antagonism seen at higher doses[66]
. Small studies have suggested efficacy, reporting 20–30% of patients achieving a significant pain reduction above placebo[67]
,[68]
. Larger studies are required before recommendations can be made in regard to the routine use of naltrexone in the management of fibromyalgia.
NMDAR inhibitors
The N-methyl-D-aspartate receptor (NMDAR) is involved in spinal cord and brain sensory pathway neural transmission via interaction with the neurotransmitter glutamate. As previously discussed, fibromyalgia patients have been shown to have elevated levels of glutamate in their central nervous system and CSF[40]
,[69]
.
Several small studies have evaluated intravenous low dose ketamine, a non-competitive NMDAR antagonist, in patients with fibromyalgia, with around half of patients experiencing a reduction in pain intensity of more than 50%[70]
. However, duration of follow up was brief and there are no long-term data for this medication.
Memantine, another non competitive NMDAR inhibitor, was evaluated in a small randomised trial in fibromyalgia and was found to be more successful than placebo at reducing pain intensity by 50%, with a number needed to treat of six[71]
. Further studies of NMDAR inhibitors in fibromyalgia are required before recommendations can be made.
Dopamine agonists
Dopamine is a neurotransmitter with multiple functions, including a central role in the modulation of pain via descending inhibitory pathways[72]
,[73]
. Using functional imaging, it was shown that fibromyalgia patients have abnormal dopaminergic activity, with reduced CNS release of dopamine in response to painful stimuli[74]
,[75]
. In a small trial, 42% of patients with fibromyalgia receiving pramipexole, a dopamine agonist, reported a 50% improvement in pain compared with 14% in placebo[76]
. However, terguride, a partial dopamine agonist, did not show any benefit[77]
. Pramipexole may also be helpful for patients with symptomatic restless leg syndrome, which is a common comorbidity with fibromyalgia[78]
. Further studies are required.
Cannabinoids
Cannabinoids are discussed as an option for management in the Canadian treatment guidelines. A recent Cochrane Review evaluated the use of cannabinoid medication in the treatment of fibromyalgia. Two studies of nabilone, a synthetic cannabinoid, were examined. Both were of very low quality and the authors concluded that there is currently no quality evidence to suggest that cannabinoids are effective for fibromyalgia symptoms[79]
.
Other experimental agents
Flupirtine is a centrally acting agent that is thought to indirectly inhibit the NMDAR by activation of the G-protein regulated inwardly rectifying potassium (GIRK) ion channel[80]
. There is evidence to suggest efficacy in acute pain, with some efficacy in fibromyalgia reported in a small case series[81],[82]
. Melatonin, an agent typically used for sleep disturbance, has also been shown to have analgesic properties, the mechanisms of which remain incompletely understood. In several small randomised trials, melatonin was shown to be superior to placebo when used either alone or in combination with other agents in treating fibromyalgia pain and sleep disturbance[83]
,[84]
,[85]
.
Conclusion
Multimodality treatment combining psychological, physical and pharmacological therapy is the best approach for patients with fibromyalgia. As discussed, medications targeting central pain pathways benefit many patients with fibromyalgia. Ongoing research into treatment options for this complex condition is required.
Financial and conflicts of interests disclosure:
The authors have no relevant affiliations or financial involvement with any organisation or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. No writing assistance was utilised in the production of this manuscript.
Reading this article counts towards your CPD
You can use the following forms to record your learning and action points from this article from Pharmaceutical Journal Publications.
Your CPD module results are stored against your account here at The Pharmaceutical Journal. You must be registered and logged into the site to do this. To review your module results, go to the ‘My Account’ tab and then ‘My CPD’.
Any training, learning or development activities that you undertake for CPD can also be recorded as evidence as part of your RPS Faculty practice-based portfolio when preparing for Faculty membership. To start your RPS Faculty journey today, access the portfolio and tools at www.rpharms.com/Faculty
If your learning was planned in advance, please click:
If your learning was spontaneous, please click:
References
[1] Clauw DJ. Fibromyalgia and related conditions. Mayo Clinic Proceedings 2015;90(5):680–692. doi: 10.1016/j.mayocp.2015.03.014
[2] Clauw DJ. Fibromyalgia: a clinical review. JAMA 2014;311(15):1547–1555. doi: 10.1001/jama.2014.3266
[3] Wolfe F, Clauw DJ, Fitzcharles MA et al. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Semin Arthritis Rheum 2016;46(3):319–329. doi: 10.1016/j.semarthrit.2016.08.012
[4] Schmidt-Wilcke T & Clauw DJ. Fibromyalgia: from pathophysiology to therapy. Nat Rev Rheumatol 2011;7(9):518–527. doi: 10.1038/nrrheum.2011.98
[5] Napadow V, LaCount L, Park K et al. Intrinsic brain connectivity in fibromyalgia is associated with chronic pain intensity. Arthritis Rheum 2010;62(8):2545–2555. doi: 10.1002/art.27497
[6] Gracely RH, Petzke F, Wolf JM et al. Functional magnetic resonance imaging evidence of augmented pain processing in fibromyalgia. Arthritis Rheum 2002;46(5):1333–1343. doi: 10.1002/art.10225
[7] Kato K, Sullivan PF, EvengÃ¥rd B et al. A population-based twin study of functional somatic syndromes. Psychol Med 2009;39(3):497–505. doi: 10.1017/s0033291708003784
[8] Gist AC, Guymer EK, Eades LE et al. Fibromyalgia remains a significant burden in rheumatoid arthritis patients in Australia. Int J Rheum Dis 2017 [Epub ahead of print]. doi: 10.1111/1756-185x.13055
[9] El-Rabbat MS, Mahmoud NK & Gheita TA. Clinical significance of fibromyalgia syndrome in different rheumatic diseases: relation to disease activity and quality of life. Reumatol Clin 2017 [Epub ahead of print]. doi: 10.1016/j.reuma.2017.02.008
[10] Guymer EK, Littlejohn GO, Brand CK et al. Fibromyalgia onset has a high impact on work ability in Australians. Intern Med J 2016;46(9):1069–1074. doi: 10.1111/imj.13135
[11] Wolfe F, Michaud K, Li T et al. EQ-5D and SF-36 quality of life measures in systemic lupus erythematosus: comparisons with rheumatoid arthritis, noninflammatory rheumatic disorders, and fibromyalgia. J Rheumatol 2010;37(2):296–304. doi: 10.3899/jrheum.090778
[12] Macfarlane GJ, Kronisch C, Dean LE et al. EULAR revised recommendations for the management of fibromyalgia. Ann Rheum Dis 2017;76(2):318–328. doi: 10.1136/annrheumdis-2016-209724
[13] Fitzcharles MA, Ste-Marie PA, Goldenberg DL et al. 2012 Canadian Guidelines for the diagnosis and management of fibromyalgia syndrome: executive summary. Pain Res Manag 2013;18(3):119–126. PMID: 23748251
[14] Bernardy K, Klose P, Busch AJ et al. Cognitive behavioural therapies for fibromyalgia. Cochrane Database Syst Rev 2013;(9):CD009796. doi: 10.1002/14651858.CD009796.pub2
[15] Busch AJ, Barber KA, Overend TJ et al. Exercise for treating fibromyalgia syndrome. Cochrane Database Syst Rev 2007;(4):CD003786. doi: 10.1002/14651858.CD003786.pub2
[16] Australian Government Depatment of Health. The Pharmaceutical Benefit Scheme. Available at: http://www.pbs.gov.au/browse/medicine-listing (accessed November 2017)
[17] US Department of Health and Human Services. US Food and Drug Administration. Available at: https://www.fda.gov/Drugs/default.htm (accessed November 2017)
[18] European Union. European Medicines Agency. Available at: http://www.ema.europa.eu/ema/ (accessed November 2017)
[19] Delgado PL. Serotonin noradrenaline reuptake inhibitors: new hope for the treatment of chronic pain. Int J Psychiatry Clin Pract 2006;10(Suppl 2):16–21. doi: 10.1080/13651500600637098
[20] Russell IJ, Vaeroy H, Javors M & Nyberg F. Cerebrospinal fluid biogenic amine metabolites in fibromyalgia/fibrositis syndrome and rheumatoid arthritis. Arthritis Rheum 1992;35(5):550–556. doi: 10.1002/art.1780350509
[21] Jones CK, Eastwood BJ, Need AB & Shannon HE. Analgesic effects of serotonergic, noradrenergic or dual reuptake inhibitors in the carrageenan test in rats: evidence for synergism between serotonergic and noradrenergic reuptake inhibition. Neuropharmacology 2006;51(7–8):1172–1180. doi: 10.1016/j.neuropharm.2006.08.005
[22] Arnold LM, Lu Y, Crofford LJ et al. A double-blind, multicenter trial comparing duloxetine with placebo in the treatment of fibromyalgia patients with or without major depressive disorder. Arthritis Rheum 2004;50(9):2974–2984. doi: 10.1002/art.20485
[23] Russell IJ, Mease PJ, Smith TR et al. Efficacy and safety of duloxetine for treatment of fibromyalgia in patients with or without major depressive disorder: results from a 6-month, randomized, double-blind, placebo-controlled, fixed-dose trial. Pain 2008;136(3):432–444. doi: 10.1016/j.pain.2008.02.024
[24] Arnold LM, Rosen A, Pritchett YL et al. A randomized, double-blind, placebo-controlled trial of duloxetine in the treatment of women with fibromyalgia with or without major depressive disorder. Pain 2005;119(1–3):5–15. doi: 10.1016/j.pain.2005.06.031
[25] Lunn MP, Hughes RA & Wiffen PJ. Duloxetine for treating painful neuropathy, chronic pain or fibromyalgia. Cochrane Database Syst Rev 2014(1):CD007115. doi: 10.1002/14651858.CD007115.pub3
[26] Mease PJ, Clauw DJ, Gendreau RM et al. The efficacy and safety of milnacipran for treatment of fibromyalgia. a randomized, double-blind, placebo-controlled trial. J Rheumatol 2009;36(2):398–409. doi: 10.3899/jrheum.080734
[27] Moret C, Charveron M, Finberg JP et al. Biochemical profile of midalcipran (F 2207), 1-phenyl-1-diethyl-aminocarbonyl-2-aminomethyl-cyclopropane (Z) hydrochloride, a potential fourth generation antidepressant drug. Neuropharmacology 1985;24(12):1211–1219. PMID: 3005901
[28] Hauser W, Clauw DJ & Fitzcharles MA. Treat-to-target strategy for fibromyalgia: opening the dialogue. Arthritis Care Res (Hoboken) 2017;69(4):462–466. doi: 10.1002/acr.22970
[29] Wang B, Yang LP, Zhang XZ et al. New insights into the structural characteristics and functional relevance of the human cytochrome P450 2D6 enzyme. Drug Metab Rev 2009;41(4):573–643. doi: 10.1080/03602530903118729
[30] Sansone RA & Sansone LA. Serotonin norepinephrine reuptake inhibitors: a pharmacological comparison. Innov Clin Neurosci 2014;11(3-4):37–42. PMID: 24800132
[31] Hall M & Buckley N. Serotonin syndrome. Australian Prescriber 2003;26(3):19. doi: 10.18773/austprescr.2003.044
[32] Park SH, Wackernah RC & Stimmel GL. Serotonin syndrome: is it a reason to avoid the use of tramadol with antidepressants? J Pharm Pract 2014;27(1):71–78. doi: 10.1177/0897190013504957
[33] Arnold LM, Hess EV, Hudson JI et al. A randomized, placebo-controlled, double-blind, flexible-dose study of fluoxetine in the treatment of women with fibromyalgia. Am J Med 2002;112(3):191–197. doi: 10.1016/S0002-9343(01)01089-0
[34] Wolfe F, Cathey MA & Hawley DJ. A double-blind placebo controlled trial of fluoxetine in fibromyalgia. Scand J Rheumatol 1994;23(5):255–259. doi: 10.3109/03009749409103725
[35] Anderberg UM, Marteinsdottir I & von Knorring L. Citalopram in patients with fibromyalgia–a randomized, double-blind, placebo-controlled study. Eur J Pain 2000;4(1):27–35. doi: 10.1053/eujp.1999.0148
[36] Patkar AA, Masand PS, Krulewicz S et al. A randomized, controlled, trial of controlled release paroxetine in fibromyalgia. Am J Med 2007;120(5):448–454. doi: 10.1016/j.amjmed.2006.06.006
[37] Walitt B, Urrútia G, Nishishinya MB et al. Selective serotonin reuptake inhibitors for fibromyalgia syndrome. Cochrane Database Syst Rev 2015(6):CD011735. doi: 10.1002/14651858.cd011735
[38] Moore A, Wiffen P & Kalso E. Antiepileptic drugs for neuropathic pain and fibromyalgia. JAMA 2014;312(2):182–183. doi: 10.1001/jama.2014.6336
[39] Fink K, Dooley DJ, Meder WP et al. Inhibition of neuronal Ca2+ influx by gabapentin and pregabalin in the human neocortex. Neuropharmacology 2002;42(2):229–236. doi: 10.1016/S0028-3908(01)00172-1
[40] Harris RE, Sundgren PC, Craig AD et al. Elevated insular glutamate in fibromyalgia is associated with experimental pain. Arthritis & Rheumatism 2009;60(10):3146–3152. doi: 10.1002/art.24849
[41] Harris RE, Napadow V, Huggins JP et al. Pregabalin rectifies aberrant brain chemistry, connectivity, and functional response in chronic pain patients. Anesthesiology 2013;119(6):1453–1464. doi: 10.1097/aln.0000000000000017
[42] Derry S, Cording M, Wiffen PJ et al. Pregabalin for pain in fibromyalgia in adults. Cochrane Database Syst Rev 2016;9:CD011790. doi: 10.1002/14651858.CD011790.pub2
[43] Arnold LM, Goldenberg DL, Stanford SB et al. Gabapentin in the treatment of fibromyalgia: a randomized, double-blind, placebo-controlled, multicenter trial. Arthritis Rheum 2007;56(4):1336–1344. doi: 10.1002/art.22457
[44] Cooper TE, Derry S, Wiffen PJ & Moore RA. Gabapentin for fibromyalgia pain in adults. Cochrane Database Syst Rev 2017;1:CD012188. doi: 10.1002/14651858.CD012188.pub2
[45] Feighner JP. Mechanism of action of antidepressant medications. J Clin Psychiatry 1999;60(Suppl 4):4–11;discussion 12–13. PMID: 10086478
[46] Carette S, Bell MJ, Reynolds WJ et al. Comparison of amitriptyline, cyclobenzaprine, and placebo in the treatment of fibromyalgia. A randomized, double-blind clinical trial. Arthritis Rheum 1994;37(1):32–40. doi: 10.1002/art.1780370106
[47] Goldenberg DL, Felson DT & Dinerman H. A randomized, controlled trial of amitriptyline and naproxen in the treatment of patients with fibromyalgia. Arthritis & Rheum 1986;29(11):1371–1377. doi: 10.1002/art.1780291110
[48] Carette S, McCain GA, Bell DA & Fam AG. Evaluation of amitriptyline in primary fibrositis. A double-blind, placebo-controlled study. Arthritis & Rheum 1986;29(5):655–659. doi: 10.1002/art.1780290510
[49] Bennett RM, Gatter RA, Campbell SM et al. A comparison of cyclobenzaprine and placebo in the management of fibrositis. A double-blind controlled study. Arthritis Rheum 1988;31(12):1535–1542. PMID: 3058130
[50] Tofferi JK, Jackson JL & O’Malley PG. Treatment of fibromyalgia with cyclobenzaprine: A meta-analysis. Arthritis Rheum 2004;51(1):9–13. doi: 10.1002/art.20076
[51] Bennett RM, Kamin M, Karim R & Rosenthal N. Tramadol and acetaminophen combination tablets in the treatment of fibromyalgia pain: a double-blind, randomized, placebo-controlled study. Am J Med 2003;114(7):537–545. doi: 10.1016/S0002-9343(03)00116-5
[52] Gong L, Stamer UM, Tzvetkov MV et al. PharmGKB summary: tramadol pathway. Pharmacogenet Genomics 2014;24(7):374–380. doi: 10.1097/FPC.0000000000000057
[53] Calandre EP, Rico-Villademoros F & Rodriguez-Lopez CM. Monotherapy or combination therapy for fibromyalgia treatment? Curr Rheumatol Rep 2012;14(6):568–575. doi: 10.1007/s11926-012-0278-y
[54] Metyas S, Ibrahim M, Ortiz E et al. THU0355 Monotherapy versus combination therapy in the treatment of fibromyalgia. Ann Rheum Dis 2013;71(Suppl 3):276. doi: 10.1136/annrheumdis-2012-eular.2320
[55] Mease PJ, Farmer MV, Palmer RH et al. Milnacipran combined with pregabalin in fibromyalgia: a randomized, open-label study evaluating the safety and efficacy of adding milnacipran in patients with incomplete response to pregabalin. Ther Adv Musculoskelet Dis 2013;5(3):113–126. doi: 10.1177/1759720x13483894
[56] Clark S, Tindall E & Bennett RM. A double blind crossover trial of prednisone versus placebo in the treatment of fibrositis. J Rheumatol 1985;12(5):980–983. PMID: 3910836
[57] Russell IJ, Fletcher EM, Michalek JE et al. Treatment of primary fibrositis/fibromyalgia syndrome with ibuprofen and alprazolam. A double-blind, placebo-controlled study. Arthritis Rheum 1991;34(5):552–560. doi: 10.1002/art.1780340507
[58] Goldenberg DL, Clauw DJ, Palmer RE & Clair AG. Opioid use in fibromyalgia: A cautionary tale. Mayo Clin Proc 2016;91(5):640–648. doi: 10.1016/j.mayocp.2016.02.002
[59] Fitzcharles MA, Faregh N, Ste-Marie PA & Shir Y. Opioid use in fibromyalgia is associated with negative health related measures in a prospective cohort study. Pain Res Treat 2013;2013:898493. doi: 10.1155/2013/898493
[60] Peng X, Robinson RL, Mease P et al. Long-term evaluation of opioid treatment in fibromyalgia. Clin J Pain 2015;31(1):7–13. doi: 10.1097/ajp.0000000000000079
[61] Harris RE, Clauw DJ, Scott DJ et al. Decreased central mu-opioid receptor availability in fibromyalgia. J Neurosci 2007;27(37):10000–10006. doi: 10.1523/jneurosci.2849-07.2007
[62] Baraniuk JN, Whalen G, Cunningham J & Clauw DJ. Cerebrospinal fluid levels of opioid peptides in fibromyalgia and chronic low back pain. BMC Musculoskelet Disord 2004;5:48. doi: 10.1186/1471-2474-5-48
[63] Brummett CM, Janda AM, Schueller CM et al. Survey criteria for fibromyalgia independently predict increased postoperative opioid consumption after lower extremity joint arthroplasty: a prospective, observational cohort study. Anesthesiology 2013;119(6):1434–1443. doi: 10.1097/ALN.0b013e3182a8eb1f
[64] Littlejohn GO, Guymer EK & Ngian GS. Is there a role for opioids in the treatment of fibromyalgia? Pain Manag 2016;6(4):347–355. doi: 10.2217/pmt-2016-0012
[65] Watkins LR, Hutchinson MR, Rice KC & Maier SF. The “toll” of opioid-induced glial activation: improving the clinical efficacy of opioids by targeting glia. Trends Pharmacol Sci 2009;30(11):581–591. doi: 10.1016/j.tips.2009.08.002
[66] Hutchinson MR, Zhang Y & Brown K. Non-stereoselective reversal of neuropathic pain by naloxone and naltrexone: involvement of toll-like receptor 4 (TLR4). Eur J Neurosci 2008;28(1):20–29. doi: 10.1111/j.1460-9568.2008.06321.x
[67] Younger J, Noor N, McCue R & Mackey S. Low-dose naltrexone for the treatment of fibromyalgia: findings of a small, randomized, double-blind, placebo-controlled, counterbalanced, crossover trial assessing daily pain levels. Arthritis Rheum 2013;65(2):529–538. doi: 10.1002/art.37734
[68] Younger J & Mackey S. Fibromyalgia symptoms are reduced by low-dose naltrexone: a pilot study. Pain Med 2009;10(4):663–672. doi: 10.1111/j.1526-4637.2009.00613.x
[69] Harris RE. Elevated excitatory neurotransmitter levels in the fibromyalgia brain. Arthritis Res Ther 2010;12(5):141. doi: 10.1186/ar3136
[70] Littlejohn G & Guymer E. Modulation of NMDA receptor activity in fibromyalgia. Biomedicines 2017;5(2):15. doi: 10.3390/biomedicines5020015
[71] Olivan-Blazquez B, Herrera-Mercadal P, Puebla-Guedea M et al. Efficacy of memantine in the treatment of fibromyalgia: a double-blind, randomised, controlled trial with 6-month follow-up. Pain 2014;155(12):2517–2525. doi: 10.1016/j.pain.2014.09.004
[72] Wood PB. Role of central dopamine in pain and analgesia. Expert Rev Neurother 2008;8(5):781–797. doi: 10.1586/14737175.8.5.781
[73] Millan MJ. Descending control of pain. Prog Neurobiol 2002;66(6):355–474. doi: 10.1016/S0301-0082(02)00009-6
[74] Wood PB, Patterson JC, Sutherland JJ et al. Reduced presynaptic dopamine activity in fibromyalgia syndrome demonstrated with positron emission tomography: a pilot study. J Pain 2007;8(1):51–58. doi: 10.1016/j.jpain.2006.05.014
[75] Wood PB, Schweinhardt P, Jaeger E et al. Fibromyalgia patients show an abnormal dopamine response to pain. Eur J Neurosci 2007;25(12):3576–3582. doi: 10.1111/j.1460-9568.2007.05623.x
[76] Holman AJ & Myers RR. A randomized, double-blind, placebo-controlled trial of pramipexole, a dopamine agonist, in patients with fibromyalgia receiving concomitant medications. Arthritis Rheum 2005;52(8):2495–2505. doi: 10.1002/art.21191
[77] Distler O, Eich W, Dokoupilova E et al. Evaluation of the efficacy and safety of terguride in patients with fibromyalgia syndrome: results of a twelve-week, multicenter, randomized, double-blind, placebo-controlled, parallel-group study. Arthritis Rheum 2010;62(1):291–300. doi: 10.1002/art.25062
[78] Montplaisir J, Nicolas A & Denesle R Gomez-Mancila B. Restless legs syndrome improved by pramipexole: a double-blind randomized trial. Neurology 1999;52(5):938–943. doi: 10.1212/WNL.52.5.938
[79] Walitt B, Klose P, Fitzcharles MA et al. Cannabinoids for fibromyalgia. Cochrane Database Syst Rev 2016;7:CD011694. doi: 10.1002/14651858.CD011694.pub2
[80] Raffa RB & Pergolizzi JV Jr. The evolving understanding of the analgesic mechanism of action of flupirtine. J Clin Pharm Ther 2012;37(1):4–6. doi: 10.1111/j.1365-2710.2010.01233.x
[81] Harish S, Bhuvana K, Bengalorkar GM & Kumar T. Flupirtine: clinical pharmacology. J Anaesthesiol Clin Pharmacol 2012;28(2):172–177. doi: 10.4103/0970-9185.94833
[82] Stoll AL. Fibromyalgia symptoms relieved by flupirtine: an open-label case series. Psychosomatics 2000;41(4):371–372. doi: 10.1176/appi.psy.41.4.371
[83] de Zanette SA, Vercelino R, Laste G et al. Melatonin analgesia is associated with improvement of the descending endogenous pain-modulating system in fibromyalgia: a phase II, randomized, double-dummy, controlled trial. BMC Pharmacol Toxicol 2014;15:40. doi: 10.1186/2050-6511-15-40
[84] Hussain SA, Al-Khalifa II, Jasim NA & Gorial FL. Adjuvant use of melatonin for treatment of fibromyalgia. J Pineal Res 2011;50(3):267–271. doi: 10.1111/j.1600-079X.2010.00836.x
[85] Citera G, Arias MA, Maldonado-Cocco JA et al. The effect of melatonin in patients with fibromyalgia: a pilot study. Clin Rheumatol 2000;19(1):9–13. doi: 10.1007/s100670050003
You may also be interested in
