Robert Matton AB / Alamy Stock Photo
Earache (otalgia) is a common presenting complaint in children. Primary otalgia, which originates in the ear, usually results from otitis externa (OE), otitis media (OM), otitis media with effusion (OME) and direct injury (see later sections for definitions and aetiology).
As the ear has a rich supply of sensory nerves from several cranial nerves, other pathologies can cause referred (secondary) otalgia. In children, these other pathologies include tonsillitis, dental disease and upper respiratory tract infection, whereas in adults, examples include dental disease, temporomandibular joint disorder (arthritis), cervical spine disease, sinusitis, or malignant disease of the neck or oral cavity.
If a patient presents with earache, a detailed history and thorough examination should help determine the underlying cause. Examination of the tympanic membrane (TM) is important in differential diagnosis and ideally would be checked to see if it is intact and mobile with pneumatic insufflation (where positive pressure is created in the ear by depressing a rubber bulb attached to an otoscope and negative pressure when the bulb is released). If the ear and TM are normal on examination, it is more likely to be secondary otalgia[1],[2],[3],[4],[5]
.
This article discusses how to diagnose and treat earache and ear infections.
Otitis externa
Definition and aetiology
OE is inflammation of the external auditory canal. The cause can be allergic, dermatological or infectious, with an acute bacterial infection being the most common aetiology. OE can occur at any age but peaks in childhood (5–14 years [USA][6]
; 7–12 years [UK][7]
) and is more common during the summer months, possibly owing to the ambient humidity and increased water activities[6]
. Swimming and other water sports, and trauma from excessive cleaning can cause maceration of the skin and breakdown of the cerumen–skin barrier, resulting in inflammation, oedema and pruritus, which can prompt scratching and cause further damage. The cerumen (earwax) in the ear is hygroscopic, meaning that it can absorb or adsorb water, and creates an acidic environment that inhibits bacterial and fungal growth[6]
. Reduced cerumen production and impaired epithelial migration raises the ears’ pH, resulting in a more favourable environment for infection.

Cotton buds or tissues should not be used to clean ears as they may become detached and can fester, becoming a focus for infection. OE is mainly diffuse, affecting the whole of the external canal, but can be localised to a hair follicle (furunclosis).
Diagnosis
Patients normally present with rapid onset of symptoms, which include:
- A red and tender ear canal, usually with a thin discharge;
- Hearing loss if the canal is very oedematous and filled with debris;
- In mild cases, minor discomfort, pruritus and oedema; and in severe cases intense pain and an occluded canal.

Source: Dr P Marazzi / Science Photo Library
Close-up of the infected outer ear (otitis externa [OE]) in a 71-year-old female patient. The skin of the external ear canal (auditory meatus) and ear pinna is cracked, red and inflamed
Treatment
Fundamental steps in the management of OE include:
- Thorough cleaning of the external canal to remove debris or wax;
- Treatment of inflammation, infection and skin conditions (eczema or psoriasis) that predispose to OE;
- Controlling pain, usually simple analgesics and non-steroidal anti-inflammatory drugs will suffice, but occasionally opioids will be necessary;
- Avoiding promoting factors, such as preventing water entering the ear by not swimming and using ear plugs or cotton wool ball with Vaseline in the shower, and no foreign bodies (e.g. cotton buds or finger nails) entering the ear. In addition, ceasing using headphones and, if possible, hearing aids during an infection;
- Following up and culturing recalcitrant cases.
The most common bacteria isolated in OE are Pseudomonas aeruginosa, Streptococcus epidermidis and Staphylococcus aureus. Fungal infection is uncommon but can occur after antibiotic treatment or in chronic OE, usually the Candida (associated with hearing aids) and Aspergillus genera are the cause. Therefore, it is important not to use a prolonged course of topical antibiotics as this may increase the risk of fungal infections[6],[8]
.
Since OE infection tends to be limited to the skin of the ear canal, treatment should be topical because a higher concentration of medication reaches the infected and inflamed tissue compared with systemic treatment. However, in patients who are immunocompromised or where the infection has spread outside the external canal, combined systemic and topical treatment is used. With furunclosis, wicks coated with glycerine and ichthammol are used, but in severe cases furuncles need to be incised and drained[5]
.
In patients who do not respond to conventional therapy, ear cultures are recommended to direct systemic antibiotic choice.
Topical treatment
- Acidifying solutions (acetic acid) or astringents (aluminium hydroxide), make the ear’s environment less conducive to bacterial growth. Acetic acid 2% (EarCalm spray®) is available over-the-counter and would be suitable in mild cases of OE;
- Antibiotics.
The addition of corticosteroids is useful in reducing inflammation, pruritus and pain. There is no robust evidence about which preparation is the most effective, however, it is imperative that ear drops are administered correctly (see ‘Box 1: how to instil ear drops’). Treatment choice is, therefore, dependent on physician preference, cost, availability and contra-indications (e.g. aminoglycosides are contra-indicated in patients with perforated ear drum, although some specialists do use them with caution, and neomycin can cause topical contact dermatitis)[6],[7],[9]
. For further information, see ‘Table 1: topical antibiotic ear drops’.
Box 1: How to instil ear drops
Pharmacists and healthcare professionals should advise patients how to appropriately administer ear drops for optimal results.
- It is recommended that the ear drops are at body temperature (hold in the hand for several minutes or put in pocket);
- Excess discharge should be mopped out of the ear but nothing should be inserted deep into the canal;
- The patient should be lying on their side, with the affected ear upmost;
- The ear should be pulled back to create a funnel, the drops instilled into the canal and the tragus (the piece of skin that sticks out just in front of the ear like a trap door) pressed to push the drops into the ear. Around 10–20 pushes should encourage the drops to reach deep into the canal;
- If there is a grommet or a perforation, the patient may be able to taste the drops owing to them travelling down the Eustachian tube;
- The patient may experience some slight dizziness, but this should settle;
- If correct positioning and tragal massaging has been performed, there is no need for the patient to lie on their side for a prolonged period.
Adapted from ENT Kent (http://entkent.com/how-to-use-ear-drops/)
A useful video can also be viewed here: https://www.youtube.com/watch?v=H-y_RZqdSzA
In severe cases of OE, where the ear canal is very swollen, ear drops cannot penetrate sufficiently down the ear canal to be effective. In these cases, a wick (compressed cotton) is inserted into the ear; it expands when drops are applied, transporting them down the ear canal. Most cases of OE improve within 48 to 72 hours and patients should have minimal symptoms at seven days, therefore, if patients fail to improve in this time-frame, the diagnosis should be re-examined[10]
. If symptoms have not totally resolved at seven days, patients can continue treatment for a total of two weeks but after this patients should be considered as treatment failures and further investigated[10],[11]
.
| Table 1: Topical antibiotic ear drops | |||
|---|---|---|---|
| Antibiotics without corticosteroids | |||
| Contra-indicated in perforated ear drum or grommets | Minimum age | General information | |
| Gentamicin 0.3% | Yes | No separate dosage for older or young patients | Prolonged use can cause skin sensitisation |
| Clotrimazole 1% Canesten | No | No separate dosage for older or young patients | Anti-fungal manufactured in propylene macrogol 400 |
| Antibiotics without corticosteroids (unlicensed or not recommended) | |||
| Quinolones Ciprofloxacin 0.3% and ofloxacin eye 0.3% drops used in the ear (unlicensed) | Unlicensed but used in perforated ear drum/grommets | Unlicensed | Non-ototoxic have been recommended in ears with grommets or perforated ear drums. Now have a licensed product (ciprofloxacin and dexamethasone) |
| Chloramphenicol 5%, 10% | Yes | Only recommended in infants if considered essential by the physician (no minimum age) | Not recommended as contains propylene glycol which is irritant. Some ear, nose and throat consultants use the eye drops in the ear (unlicensed) |
| Antibiotics with corticosteroids | |||
| Ciprofloxacin and dexamethasone 0.3%/0.1% Cilodex | No | Six months acute otitis externa (OE) and one year for acute otitis media (OM) in patients with tubes but can be used in younger patients at discretion of physician | Not applicable |
| Clioquinol and flumetasone 0.02%/1% | Yes | Two years | Previously launched as Locorten-vioform® now only available as a generic. Claimed to have an anti-fungal and antibacterial activity. May interfere with some laboratory tests |
| Framycetin, gramicidin and dexamethasone 0.5%/0.05% and 0.005% Sofradex | Yes | No separate dosage for older or young patients | May cause hypersensitivity with prolonged use |
| Gentamicin and hydrocortisone 0.3%/1% Gentisone HC | Yes | No separate dosage for older or young patients | May cause hypersensitivity with prolonged use |
| Neomycin with betamethasone 0.1%/0.385% | Yes | No separate dosage for older or young patients | May cause hypersensitivity with prolonged use |
| Neomycin, dexamethasone and glacial acetic acid 0.5%/0.1%/2% Otomize | Yes | Not to be used in children under two years of age | May cause hypersensitivity with prolonged use |
| Unlicensed combination products | |||
| Triamcinolone, Nystatin, neomycin and gramicidin 0.1%/100,000 units/0.25%/0.025% | Yes | One year | Previously tri-adcortyl otic ointment. Discontinued in the UK but available as an import or unlicensed special |
| Sources: BNF legacy and summary of product characteristics of individual products. | |||
Necrotising otitis externa (NOE), previously called malignant OE, is a potentially life-threatening complication of OE where the infection spreads to the skull base. It is usually caused by a Pseudomonal infection and is associated with older patients, patients with poorly controlled diabetes or immunosupressed patients. Patients with NOE will require urgent specialist treatment[6],[7],[9],[10]
.
Otitis media
In OM, the middle ear is filled with fluid[12]
. In acute otitis media (AOM) the fluid is infected, whereas it is not infected in OME. OME can either proceed or follow AOM. It can be difficult to correctly differentiate OME and AOM as they are part of a continuous spectrum. However, it is important to diagnose them appropriately because treatment is different.
AOM
Definition and aetiology
AOM is the commonest bacterial condition in infants and young children. It peaks between 6 and 18 months, and there is a smaller subsequent peak around 5 to 6 years of age[4],[13]
. It is characterised by middle ear effusion and TM inflammation. The latter is usually white or pale yellow and bulges out into the external auditory canal, and has absent or limited mobility.

Source: Dr P Marazzi / Science Photo Library
Close-up of the ear of a 14-month-old boy suffering from otitis media with a perforated eardrum. Otitis media is an inflammation of the middle ear. In this case the eardrum (tympanum) has burst resulting in a discharge of pus (yellow liquid)
AOM is often associated with a viral upper respiratory tract infection, which can cause inflammation and obstruction of the Eustachian tube. This inflammation and obstruction causes a negative pressure in the middle ear, resulting in accumulation of fluid that can be colonised by bacteria and viruses. With microbial growth suppuration (forming of pus) occurs, producing the bulging ear drum, which can occasionally perforate leading to a profuse and mucopurulent discharge. The most commonly isolated bacteria are Streptoccocus pneumonia, Haemophilius influenzae and Moxarella
catarrhalis
[4],[13],[14]
.
Risk factors for AOM include passive smoking[13],[14]
. Vaccination against pneumococcal strains can provide some protection[13],[14]
.
Diagnosis
Symptoms can include earache, hearing loss, fever, headache, anorexia, vomiting and diarrhoea[13]
. AOM is usually diagnosed using an otoscope.
Treatment
Around 80% of cases of AOM in children resolve within three days with no antibiotic treatment[14]
, therefore, most patients should be given supportive treatment with analgesia rather than immediate antibiotics. However, if there is no resolution after four days, oral antibiotics should be prescribed, although the evidence for effectiveness remains unclear[15],[16]
. Immediate treatment with antibiotics are recommended for:
- Patients younger than two years of age with bilateral AOM;
- Patients with perforation and/or discharge in the ear;
- Patients who are at high risk of complications (e.g. immunosuppressed or have significant heart, lung disease etc.);
- Patients who are systemically unwell but do not require admission to hospital.
Children under the age of six months with a very high temperature and patients showing any signs of complication (e.g. mastoiditis, nerve palsy, meningitis) should be referred immediately to secondary care.
If antibiotics are prescribed, the treatment of choice is amoxicillin for five days or clarithromycin/erythromycin if the patient is allergic to penicillin[14]
. Co-amoxiclav is a second-line antibiotic for treatment failures[14]
.
Complications
In rare cases, AMO can develop into a chronic suppurative otitis media (CSOM), which presents as a recurrent discharge through the TM. The WHO defines CSOM as recurrent discharge for more than two weeks[17],[18]
, but some experts define it as more than six weeks[17]
. In CSMO, the ear is usually painless but loss of hearing can occur and if left untreated complications, such as facial paralysis, mastoiditis, cholesteatoma (a keratinised mass in the middle ear), meningitis or cranial abscess may occur[19]
. Although these are rare complications, occurring in 0.7–3.2% of patients[20]
, owing to their seriousness, patients should be treated in secondary care[17]
.
In CSOM, the ear should be thoroughly cleaned to reduce the quantity of infected material and allow better penetration of ear drops. Topical treatment is the treatment of choice, as penetration through the devascularised mucosa of the middle ear and the mastoid is poor with systemic treatment. Although evidence of the efficacy of treatments for CSMO is not robust, there is reasonable evidence to support the use of quinolones and, unlike aminoglycosides, they are non-ototoxic[17],[21]
. Systemic treatment should, however, be added in patients at risk of complications or those who fail to respond after two to three weeks of topical therapy. Surgery may be necessary in some patients to remove infected tissue and repair ear damage[17]
.
Otitis media with effusion (OME)
Definition and aetiology
Commonly known as “glue ear”, the main presenting feature of OME is a conductive hearing loss. It is very common in children (80% having at least one episode by the age of ten), with a bimodal peak at two and five years of age, is more common in winter months and usually lasts six to ten weeks[22]
. It is also very common in children with Down’s syndrome or cleft palate[22],[23]
.
Diagnosis
Otoscopic examination of OME shows a dull and often retracted TM, which may be immobile. Most cases respond spontaneously but some children will need specialist interventions due to the hearing loss causing educational problems.
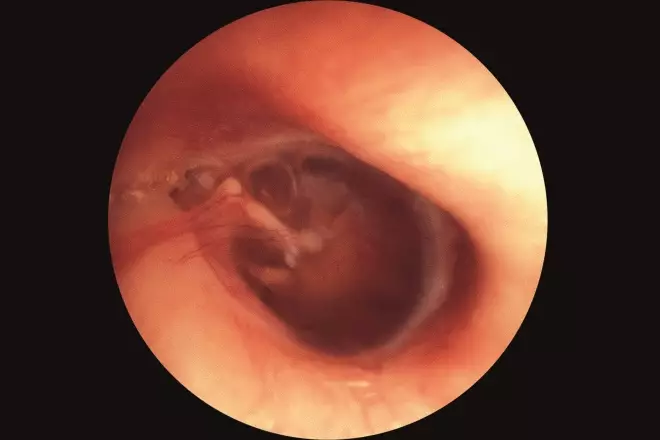
Source: Clinica Claros, ISM / Science Photo Library
Otoscopy image of the interior of the ear of a child affected by otitis media with effusion (OME), commonly referred to as glue ear. It is a collection of fluid (effusion) that occurs within the middle-ear space due to the negative pressure produced by dysfunction of the Eustachian tube
Treatment
The National Institute for Health and Care Excellence (NICE), England’s health technology assessment body, recommend surgery (myringotomy and insertion of a ventilation tube ‘grommet’) for children under 12 years of age who have had persistent documented OME of over three months, with a hearing level in the better ear of 25dBHl–30dBHl or worse[23]
. There is a proviso that children who do not fulfil the criteria can have surgery where the impact of the hearing loss on the child’s development is judged to be significant. Adjuvent adenoidectomy is only recommended in patients with persistent or frequent upper respiratory tract symptoms.
Hearing aids are useful in some cases and clinical trials have demonstrated significant improvement in middle ear function in children treated with autoinflation (latex balloons inflated by blowing through the nose) provided children can comply with the treatment[24]
.
As no conclusive benefit has been demonstrated for the use of topical or systemic antihistamines, topical or systemic antibiotics, topical or systemic steroids, probiotics and alternative treatments, these are not recommended[22],[23]
.
Other common ear complaints
Object in the ear
Foreign bodies in the ear canal are normally found in children. Items that can cause severe damage (e.g. batteries and penetrating foreign bodies, such as hair pins or cotton buds) need urgent removal. Insects should be killed with either mineral oil or lidocaine before removal[25]
. See box 2 for additional resources on earache from NICE.
Ear wax
Cerumen impaction, a build-up of ear wax, is more common in older patients. It is a common cause of discomfort but rarely causes intense pain. Eardrops should be recommended to soften it so that it falls out naturally (see box 1 for information about how to administer ear drops).
Box 2: Additional resources
- National Institute for Health and Care Excellence (NICE). Clinical knowledge summary. Otitis media – acute
- NICE. Clinical knowledge summary. Otitis externa
- NICE. Clinical knowledge summary. Earwax
- NICE. Clinical knowledge summary. Otitis media with effusion
- NICE. Clinical knowledge summary. Otitis media – chronic suppurative
Reading this article counts towards your CPD
You can use the following forms to record your learning and action points from this article from Pharmaceutical Journal Publications.
Your CPD module results are stored against your account here at The Pharmaceutical Journal. You must be registered and logged into the site to do this. To review your module results, go to the ‘My Account’ tab and then ‘My CPD’.
Any training, learning or development activities that you undertake for CPD can also be recorded as evidence as part of your RPS Faculty practice-based portfolio when preparing for Faculty membership. To start your RPS Faculty journey today, access the portfolio and tools at www.rpharms.com/Faculty
If your learning was planned in advance, please click:
If your learning was spontaneous, please click:
References
[1] Dhillon R & East C. Ear, nose and throat and head and neck surgery. 2nd edition, Churchill Livingstone.
[2] Ely J, Hanson M & Clark E. Diagnosis of ear pain. Am Fam Physician 2008;77(5):621–628. PMID: 18350760
[3] Li J & Myers A. Otalgia. Medscape. Available at: http://emedicine.medscape.com/article/845173-overview?pa=h7P4KC6ihJNTibOE5PCr4MLCBWm4PwNawo1KyrcSGDzlW3Mrt4YJs5hKxsuH2ek16DpUuNk9NMEKT%2BGX7ibOI%2Ban9ne3zvU8w6HMSMo32z4%3D (accessed April 2017)
[4] Majumdar S, Wu K, Bateman ND & Ray J. Diagnosis and management of otalgia in children. Arch Dis Child Educ Pract Ed 2009;94:33–36. doi: 10.1136/adc.2007.117994
[5] Ludman H. ABC of otolaryngology. BMJ publishing group 4th Edition.
[6] Gougen L. External otitis: pathogenesis, clinical features and diagnosis. Uptodate.com. Available at: https://www.uptodate.com/contents/external-otitis-pathogenesis-clinical-features-and-diagnosis (accessed April 2017)
[7] National Institute for Health and Care Excellence (NICE). Clinical knowledge summary. Otitis externa. Available at: https://cks.nice.org.uk/otitis-externa#!topicsummary (accessed April 2017)
[8] Sander R. Otitis externa: a practical guide to treatment and prevention. Am Fam Physician. 2001;63(5):927–937. PMID: 11261868
[9] Gougen L. External otitis treatment. Uptodate.com. Available at: https://www.uptodate.com/contents/external-otitis-treatment?search=otitis%20externa%20treatment (accessed April 2017)
[10] Rosenfeld RM, Schwartz SR, Cannon CR et al. Clinical practice guideline: acute otitis externa executive summary. Otolaryngol Head Neck Surg 2014;150(2):161–168. doi: 10.1177/0194599813517659
[11] Kaushik V, Malik T & Saeed AR. Interventions for acute otitis externa. Cochrane Database Syst Rev. 2010;CD004740. doi: 10.1002/14651858.CD004740.pub2
[12] Wald E. Acute otitis media in children. Diagnosis. Uptodate.com. 2016. https://www.uptodate.com/contents/acute-otitis-media-in-children-diagnosis?source=search_result&search=otitis%20media&selectedTitle=3~150 (accessed April 2017)
[13] Klein J & Pelton S. Acute otitis media in children: epidemiology, microbiology, clinical manifestations and complications. Uptodate.com. 2016. Available at: https://www.uptodate.com/contents/acute-otitis-media-in-children-epidemiology-microbiology-clinical-manifestations-and-complications?source=search_result&search=acute%20otitis%20media&selectedTitle=3~150 (accessed April 2017)
[14] NICE. Clinical knowledge summary. Otitis Media acute. Available at: https://cks.nice.org.uk/otitis-media-acute#!topicsummary (accessed April 2017)
[15] Klein J & Pelton S. Acute otitis media in children: treatment. Uptodate.com. Available at: https://www.uptodate.com/contents/acute-otitis-media-in-children-treatment?source=see_link (accessed April 2017)
[16] Venekamp RP, Sanders SL, Glasziou PP et al. Antibiotics for acute otitis media in children. Cochrane Database Syst Rev 2015;CD000219. doi: 10.1002/14651858.CD000219.pub4
[17] Lustig L, Limb C, Baden R & LaSalvia M. Chronic otitis media, cholesteamota, and mastoiditis in adults. Uptodate.com. Available at: https://www.uptodate.com/contents/chronic-otitis-media-cholesteatoma-and-mastoiditis-in-adults?source=see_link (accessed April 2017)
[18] World Health Organization. Chronic suppurative otitis media. Burden of illness and management options. Available at: http://www.who.int/pbd/publications/Chronicsuppurativeotitis_media.pdf (accessed April 2017)
[19] Limb C, Lustig L & Klein J. Acute otitis in adults (suppurative and serous). Uptodate.com. 2017. Available at: https://www.uptodate.com/contents/acute-otitis-media-in-adults-suppurative-and-serous (accessed April 2017)
[20] NICE. Clinical knowledge summary. Otitis media — chronic suppurative. Available at: https://cks.nice.org.uk/otitis-media-chronic-suppurative#!topicsummary (accessed April 2017)
[21] Coates H. Ear drops and ototoxicity. Aust Prescr 2008;31:40–41. doi: 10.18773/austprescr.2008.024
[22] NICE. Clinical knowledge summary. Otitis media with effusion. Available at: https://cks.nice.org.uk/otitis-media-with-effusion#!topicsummary (accessed April 2017)
[23] NICE. Clinical guideline [CG60]. Otitis media with effusion in under 12s: surgery. Available at: https://www.nice.org.uk/Guidance/CG60 (accessed April 2017)
[24] NICE. Medtech innovation briefing [MIB59]. Otovent nasal balloon for otitis media with effusion. Available at: https://www.nice.org.uk/advice/mib59 (accessed April 2017)
[25] Isaacson G & Ojo A. Diagnosis and management of foreign bodies of the outer ear. Uptodate.com. Available at: https://www.uptodate.com/contents/diagnosis-and-management-of-foreign-bodies-of-the-outer-ear?source=see_link (accessed April 2017)