

In 2006–07 the NHS in England spent £10.6bn on medicines.However, around £300m worth of prescription medicines are wasted in England per year and up to 50% of medicines prescribed for long-term conditions are not taken as recommended.1,2
Although pharmacists routinely address practical barriers to help patients optimise their medication (for example, through medicines use reviews), non-adherence remains a substantial problem. So how come patients do not take their medicines as intended? And what more can we do to support them in doing so?
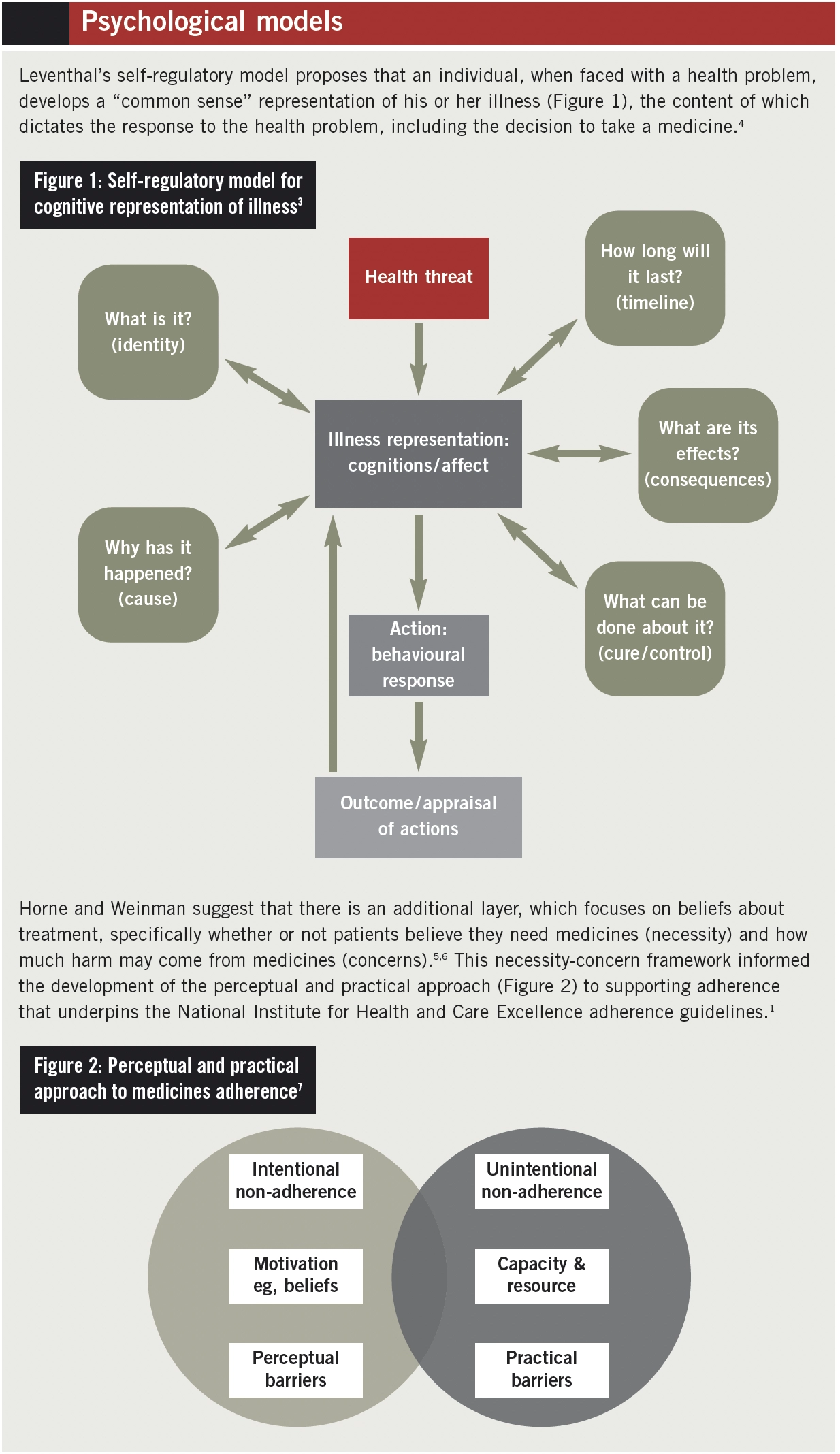
Psychological models can be used to consider how patients deal with health problems, and these theories are described in the Box on p86. The challenge is knowing how to incorporate these theoretical models into everyday pharmacy practice to improve patient adherence.
A patient’s view
In 2011, consultant pharmacist for older people Nina Barnett described her own experiences of being a patient, and her struggle with issues around adherence (Pharmaceutical Journal 2011;287:201). She shared her thoughts around her proposed vitamin D prescription, which included:
- What good will a supplement do me?
- How will I remember to take it twice a week, let alone forever?
- This is a life sentence of regular medication
- I feel fine — I don’t need tablets
She also expressed some anger about the situation, despite her professional knowledge that “should” have led her to feel otherwise.
If we were to use the perceptual and practical approach (see Box, p86) to consider Mrs Barnett’s case, we can see that her first two statements relate to the practicalities of taking a medicine and the last two statements are based on her perceptions. Pharmacists are already adept at addressing practical barriers to medicines taking and I believe that these skills can be extended to include tackling the perceptual barriers to adherence.
Lessons from CBT
Cognitive behavioural therapy (CBT) was developed by Aaron Beck and colleagues, who proposed that people hold core beliefs about themselves, others and the world, through which everyday events are interpreted, and mood and actions dictated (the cognitive-behavioural model).7
CBT is a discrete, time-limited, structured psychological intervention in which a patient works collaboratively with a therapist to identify the content and effects of their thoughts, beliefs and emotional states. As a pharmacist and CBT therapist, I have previously led drop-in clinics on adult mental health wards and the day centre at Oxford Health NHS Trust, which ran for one hour per week. Patients self-referred for 10-minute appointments and discussed any issues they had regarding their medicines — the patients set the agenda.
The consultations were conducted using CBT principles and strategies, exploring both practical and perceptual barriers to adherence. The CBT model supports medicines adherence guidance from the National Institute for Health and Care Excellence, which recommends that healthcare professionals elicit and address patient concerns and preferences around medicines. I believe that this advice can be readily translated to general, patient-facing pharmacy practice.
CBT in pharmacy practice
Returning to the case above, it is likely that Mrs Barnett’s practical concerns would be addressed in a routine pharmacist interaction. One of her perceptual concerns, the fact that she did not believe that she needed the medicine (“I feel fine”), might also be addressed. Without a prompt to express such ideas, she was left to wrestle with her thoughts and feelings about the new prescription.
Focusing specifically on her perceptions about the prescribed medicine (the latter two statements), a CBT approach to the consultation could include the following:
- Normalising statements — for example: “Having to take medicines long term can be quite a big change for many people, especially when you feel healthy and well, so it is quite normal to have concerns or to feel sceptical/angry/nervous/hurt, etc”
- Sensitive probing questions to elicit concerns — for example: “What concerns do you have about your prescription/illness/condition?”; or “What bothers you most about having to take these medicines?”
- Empathy, reflection and provision of a rationale for continued questions — for example: “It sounds like you are quite worried and unsure about taking these tablets; this is quite natural but sometimes these ideas can get in the way of you getting the most out of your medicines”
- Addressing questions — “When we are feeling worried or unsure it is natural to jump to the worst conclusions or to discount any positives that might occur. What do you think is the worst that will happen? What convinces you that these ideas are true? What about the very best outcome? What do you think is the most realistic outcome?” (At this point, the pharmacist might need to offer more medication counselling if the patient is struggling to answer the questions)
Strategies and techniques used in CBT are similar to other approaches such as health coaching, which aims to raise patient awareness and increase patient responsibility for their health, including medicines taking.8,9
The questions and techniques used in both approaches seek to elicit and explain existing difficulties, explore alternatives, develop new courses of action and empower individuals to implement them.
Summing up
My experience suggests that CBT principles and techniques can be used as part of routine pharmacy practice in short consultations to improve medicines adherence.
I believe that practical and perceptual barriers to medicines taking can be better addressed by incorporating a CBT-based approach to questioning as part of routine interactions with patients, such as medicines use reviews in community pharmacy or discharge medication counselling in hospitals.
Acknowledgement
Thanks to Nina Barnett, consultant pharmacist for the care of older people at East and South East England Specialist Pharmacy Services.
References
- National Institute for Health and Clinical Excellence. Medicines Adherence: involving patients in decisions about prescribed medicines and supporting adherence. January 2009. www.nice.org.uk/cg76 (accessed 25 October 2012).
- Trueman P, Lowson K, Blighe A, et al. Evaluation of the scale, causes and costs of waste medicines: final report. London and York: School of Pharmacy, University of London, report, York Health Economics Consortium; 2010.
- Scott J, Tacchi MJ. A pilot study of concordance therapy for individuals with bipolar disorders who are non-adherent with lithium prophylaxis. Bipolar Disorders 2002;4:386–92.
- Leventhal H, Diefenbach M, Leventhal EA. Illness cognition: using commons sense to understand treatment adherence and affect cognition interactions. Cognitive Therapy and Research 1992;16:143–63.
- Horne R, Weinman J. Patient’s beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. Journal of Psychosomatic Research 1999;47:555–67.
- Horne R, Weinman J, Barber N, et al. Concordance, adherence and compliance in medicines-taking. Report for the National Co-ordinating Centre for NHS Service Delivery and Organisation R&D. 2005.
- Beck, AT. Cognitive therapy and the emotional disorders. New York: Penguin; 1976.
- Barnett NL. The new medicines service and beyond — taking concordance to the next level. Pharmaceutical Journal 2011;287:653.
- Barnett NL, Sanghani P. A coaching approach to improving concordance. International Journal of Pharmacy Practice. Online 20 November 2012.


