

Key points
- Evidence shows pharmacists’ interventions, in collaboration with other healthcare professionals, improve type 2 diabetes mellitus (T2DM) management outcomes. However, it is not clear whether the seven targeted areas, as stipulated in national and international diabetes guidelines, were addressed.
- In this study, pharmacists without formal diabetes training were upskilled to apply the novel Simpler tool to facilitate delivery of T2DM interventions.
- The multifaceted tool consisted of seven targeted areas to deliver guideline-specific diabetes care instead of a single or dual ill-defined intervention, as documented in numerous studies.
- The tool structured pharmacist interventions to the prescriber and assisted patients’ self-management to improve quality of life outcomes among patients with T2DM.
Introduction
In 2017, 425 million people worldwide had diabetes, of which 80% of people with diabetes resided in low- or middle-income countries, such as Malaysia[1]
. The 2013 Malaysia DiabCare study reported that of the 1,688 patients with diabetes studied, 15.7% had angina and 18.4% had suffered a myocardial infarction[2]. In addition, 41% had neuropathy and 31.5% had cataracts[2]
. The 2015 Malaysian ‘National Health and Morbidity Survey’ found that the prevalence of all types of diabetes was 17.5%[3]
. Therefore, healthcare professionals should understand the need for appropriate glycaemic control and measures to prevent long-term diabetes complications.
National and international guidelines for the management of type 2 diabetes mellitus (T2DM), including those produced in Australia, Malaysia, the UK and the United States, as well as from the International Diabetes Federation, identify seven targeted areas of care, which are:
- Glycaemic control;
- Cholesterol control;
- Blood pressure;
- Medicine;
- Lifestyle;
- Cardiovascular risk reduction management;
- Patient education[4],[5],[6],[7],[8]
.
However, it is unclear if all seven areas have been addressed in studies that have reported beneficial outcomes owing to pharmacists’ provision of diabetes care[9]
.
This study examined pharmacists’ interventions and education, as well as quality of life (QOL)-related data, as part of a large randomised controlled trial (RCT) conducted in seven primary care clinics in the state of Johor, Malaysia. These clinics are publicly funded, government-managed institutions that provide ambulatory care. Malaysian citizens pay a subsidised amount of RM1 (US$0.23) for a doctor’s consultation and medicine costs for the duration of treatment. The primary care team consists of doctors, family medicine specialists, dentists, pharmacists, nurses and dietitians.
The Simpler diabetes intervention tool
This validated tool encompasses the seven targeted areas for diabetes care and their corresponding indicators with the aim of facilitating the delivery of structured, multifaceted interventions to provide consistent-quality T2DM care.
The development and validation of the Simpler tool was conducted in 2014[10]
. In phase one of the project, a Delphi method was used to validate the tool by obtaining consensus from 12 diabetes experts (pharmacists, doctors, endocrinologists and diabetes nurses) from Australia and Malaysia. The indicators were then categorised into seven broad treatment areas derived from T2DM guidelines from Australia, Malaysia, the UK, US and large RCTs. Of the 38 indicators within the seven areas presented to the panel, 94.7% (n=36) achieved consensus level at 60%[10]
. The tool’s targeted areas and the corresponding indicators are presented in Table 1.
Phase two was conducted in 2015 and involved development and evaluation of the Simpler training package, and training of pharmacists (n=12) from community practice in Australia and primary healthcare clinics in Malaysia. Participants’ feedback on the tool was applied to refine the tool and the training package as outlined in the reference[11]
.
Assessing quality of life
The World Health Organization (WHO) defines QOL as a person’s perception of their life in the culture and system where they live associated with their life’s goals, expectations and concerns[12]
. QOL scores reflect a person’s ability to self-manage their condition[4]
.
A higher QOL score is associated with better clinical outcomes and less anxiety about the condition[12]
. A lower diabetes QOL score has been found among patients with multiple comorbidities[13],[14]
. The WHOQOL-BREF is an abbreviated 26-item questionnaire to assess individual’s perceptions in relation to their goals, expectations, standards and concerns[12]
. It consists of four domains — namely physical health, psychological, social relationships and environment.
Aims
The aim of this study was to evaluate the application of the Simpler tool in the management of patients with T2DM to:
- Determine the types and effectiveness of medicine-related and education interventions conducted by pharmacists in collaboration with patients and healthcare professionals;
- Evaluate the impact of the interventions on patients’ QOL.
The outcomes related to glycaemic, blood pressure and cholesterol results have been published elsewhere[15]
.
Ethical considerations
This study was approved by the Curtin University Human Research Ethics Committee and the Malaysian Medical Research and Ethics Committee. The trial was registered with the National Medical Research Register of Malaysia under the title of ‘Development and evaluation of a pharmacist diabetes intervention tool: a mixed methods study’.
Methods
This study was a two-arm, single-blinded, six-month patient follow-up trial conducted between June 2016 and February 2017. Patient recruitment was conducted between June and September 2016. The detailed method of the larger RCT has been previously described[15]
.
Patient recruitment
Patients were recruited at seven primary healthcare clinics located in the state of Johor, Malaysia. The inclusion criteria for the patients were: T2DM diagnosis; aged >21 years (as required by the Malaysian Medical Research and Ethics Committee); takes multiple medicines/ has multiple comorbidities; and HbA1c >8% (63.9mmol/mol) or average blood glucose >10mmol/L. Exclusion criteria were: diagnosed with dementia or severe psychotic illness; on haemodialysis treatment; pregnant or lactating; intending to be pregnant within the next six months; diagnosed with cancer; or were involved in other research at the time of recruitment. Patients who were previously recruited into other medicine management services, such as the diabetes medication therapy adherence clinic (DMTAC) prior to the start of the trial, were also excluded. This was to minimise the possibility of bias as patients with previous exposure to DMTAC were judged to possibly have increased knowledge of diabetes self-management in comparison to other patients.
Patient recruitment processes were conducted either through seeking consent from patients who visited the pharmacy and fulfilled the inclusion criteria, or through referral by diabetes nurses. Patients were blinded; however, the pharmacists knew which arm patients were randomised to.
There were two arms (see Figure 1):
- The intervention arm, Simpler care (SC): this involved patients receiving care from pharmacists applying the Simpler tool, in addition to routine care from doctors, diabetes nurses and, if necessary, dieticians;
- The control arm, usual care (UC): this involved patients receiving routine care only. Routine care consisted of patients having a quarterly 20-minute appointment with a doctor, 10 minutes with a diabetes nurse and, if necessary, 20 minutes with a dietician, as well as a monthly 10-minute visit with the dispensing pharmacists for medication provision.
SC patients were followed up every month for a period of six months by the intervention pharmacist, while UC patients were seen once at the beginning of the trial and again at the end of the trial (at six months, week 27) for data collection. This method follows similar published RCT studies[9]
.
Intervention arm patients
Consultation with SC patients by the intervention pharmacists was of 20–30 minutes duration. Pharmacists made assessments from information gathered from patients and medical records. Subsequently, using the Simpler tool, they documented their interventions and individual goals for patients, and these were evaluated at each following visit.
The Simpler tool prompted pharmacists to make interventions and forms were used in the documentation process. Form A was used on days when patients had appointments with a doctor and nurse; the doctors were encouraged to record their interventions on the form using black ink while nurses used blue ink and pharmacists, purple ink. Form B was used when patients only had an appointment with the pharmacist and then attached to the patients’ medical notes.
Pharmacists used the tool to identify the appropriate therapy and make recommendations to the prescriber. In addition, they could adjust insulin dosages within defined limits, as agreed in the trial protocol. Patients were seen in a private consultation room when they had a doctor’s appointment and, otherwise, at a private counselling area at the pharmacy. An audit was performed on completed forms by the researcher to ensure the required information was recorded.
Patients completed the self-administered abbreviated version of the WHO QOL 100 assessment (WHOQOL-BREF) anonymously in the Bahasa Malaysia language, which had previously been validated in Malaysia[16]
. The questionnaire was administered to patients at the start (visit one) and at the end (visit six) of the study. The overall scores comprise of questions on self-evaluation of QOL and self-assessment of health.
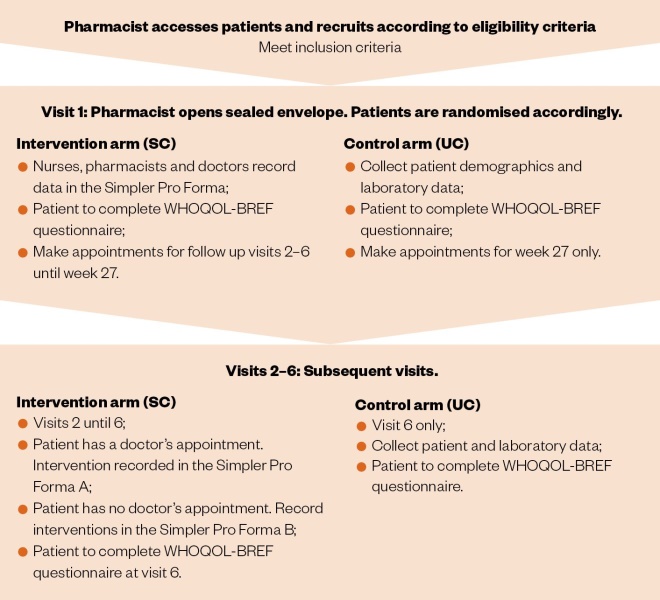
Figure 1: Flow diagram of the process involved in the intervention and control arms
Pharmacist recruitment and training
The eligibility criteria for pharmacists included having up to three years of clinical experience in diabetes management, as well as not having undergone the credentialing process to become a credentialed diabetes pharmacist by the Pharmaceutical Services Division, Ministry of Health, Malaysia. The rationale was to limit the possibility of pharmacists’ diabetes management knowledge and skills being due to prior training or years of clinical experience. Pharmacists from 11 primary healthcare clinics from 6 of 10 districts in the state of Johor, Malaysia, who fulfilled the inclusion criteria, were contacted by email and telephone. Pharmacist participation was voluntary, and two pharmacists were recruited from each clinic to ensure cover for absences owing to holidays, sickness or other reasons.
Participating pharmacists were required to complete a two-hour training programme on diabetes management incorporating the Simpler tool. Training commenced once they signed consent forms to participate in the research, which had to be completed before the start of the trial. This was to ensure uniformity in skills set among the pharmacists, as suggested in previous literature[17]
. In addition, current diabetes management information was sent to pharmacists periodically by the researcher to keep them informed of recent developments.
All interventions were recorded in Form A and B. The types of interventions and topics for the education provided followed the indicators in the Simpler tool and are summarised in Table 1, and also includes the evaluation tools used.
Table 1. The data evaluated and education topics using the Simpler tool | |||
| Targeted areas | Indicators | Data evaluated | Indicators used as education topics |
| S – Statin |
|
|
|
| I– Insulin/glycaemic control |
|
|
|
| M – Medication |
|
|
|
| P – Blood pressure |
|
|
|
| L– Lifestyle |
|
|
|
| E– Education |
|
| |
| R– Cardiovascular risk |
|
|
|
| ACEI: angiotensin-converting enzyme inhibitor; ARB: angiotensin receptor blocker; BMI: body mass index; BP: blood pressure; CVD: cardiovascular disease; HbA1c: glycated haemoglobin; LDL: low density lipoprotein; MCQ: medication compliance questionnaire; PDE-5 inhibitor: phosphodiesterase-5 inhibitor; SMBG: self-monitoring of blood glucose; TG: triglyceride; QOL: quality of life; WHOQOL-BREF: abbreviated quality of life scale developed through World Health Organization. | |||
Results
A total of 14 pharmacists from 7 clinics agreed to participate. Most pharmacists (71.4%; n=10) had been conducting diabetes management services for less than one year, and the remainder (28.6%; n=4) had been doing so for less than three years.
There were 77 SC and 77 UC patients recruited. Of the 77 SC patients, 21% (n=16) did not complete the study as they did not attend the final follow-up visit, while 8% (n=6) completed only two visits. A required minimum of three visits for SC patients were required, as this was one visit more than the control patients. In addition, it allowed patient education on various aspects of diabetes medication and self-management to occur throughout the trial period. Therefore, the analysis of results included data for 71.4% (n=55) of SC patients that completed the study and who attended a minimum of three visits, further to 89.6% (n=69) of UC patients who completed the required two visits. Table 2 presents patients’ baseline data and demographic background.
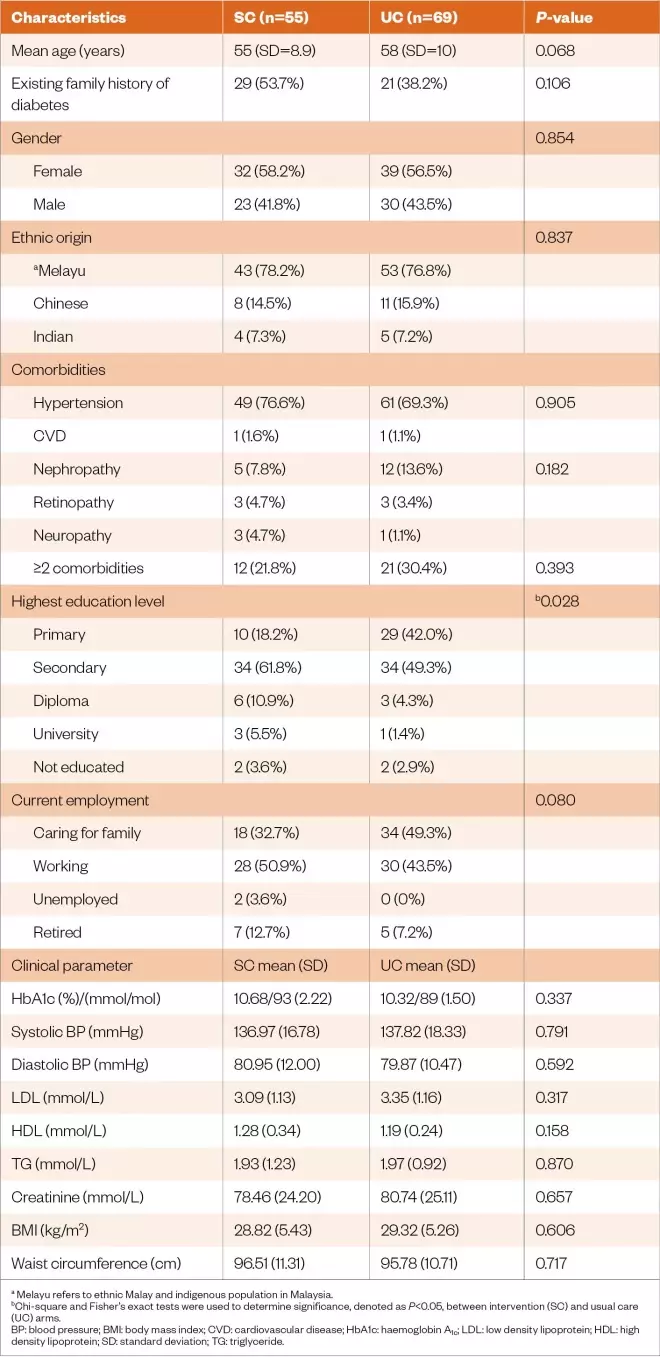
Table 2: Baseline characteristics of the study population
Medication management interventions
Patient medication lists included mostly antidiabetic, antihypertensive, lipid lowering and antiplatelets, as well as those presented in Table 3.
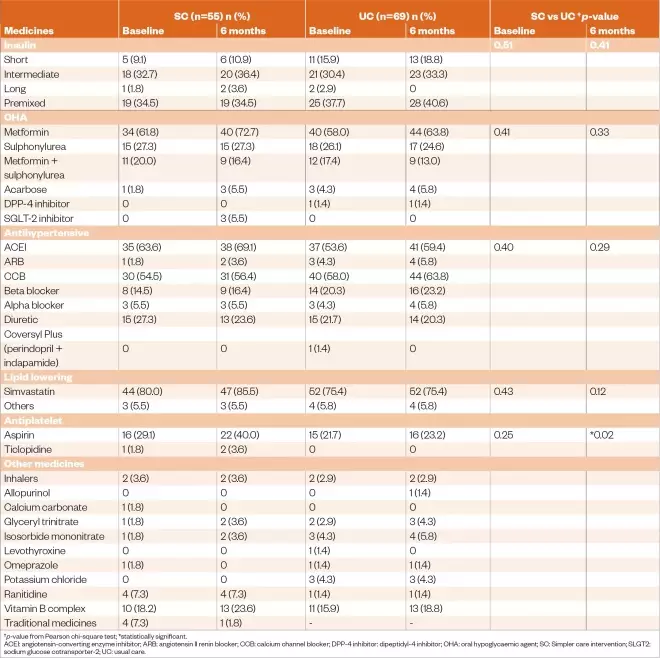
Table 3: Medication use and changes made over six months in the Simpler care and usual care arms
The number of patients who were prescribed metformin increased slightly at six months for both the Simpler care (10.7%) and usual care (6%) arms. However, the differences between groups were not statistically significant at baseline (P =0.408) and six months (P =0.337). Similarly, there was a non-significant increase in the number of patients prescribed insulin between groups at six months (P =0.414).
The SC arm had a non-significant increase (5.4%; n=47) in the number of patients on prescribed insulin at six months compared to baseline, while the UC arm had an increase of 2.9% (n=64). Similarly, the SC arm had a non-significant higher proportion of patients (74.5%) on insulin, as required by the Malaysian diabetes guidelines, when compared to the UC arm (72.5%) at six months. The same guidelines recommend insulin initiation if patients present with uncontrolled diabetes, despite being on two or more oral diabetes medicines[6]
.
Pharmacist intervention on the initiation of angiotensin-converting enzyme inhibitor (ACEI) and angiotensin II renin blocker (ARB) contributed to a slight increase (11%; n=X) in prescribed ACEI for the SC group at the end of the study at six months; however, this increase was not statistically significant (baseline versus six months). Equally, UC patients had a non-significant increase, (12.5%) of prescribed ACEI/ARB at six months. The SC group had a significantly (P=0.016) increased number of total antiplatelet medicines prescribed at the end of the study in comparison with the UC group.
Medicine-related problems
The most common medicine-related problem (MRP) was patients’ non-adherence, which accounted for 44.9% (n=135/301) of MRPs. The most frequent causes of non-adherence to medicines were patients forgetting to take their medicine (68.1%; n=124/182), followed by patients preferring not to take their medicine (23.1%; n=42/182). Overall, there were 1.3% (n=4) recordings of adverse drug reactions, which were related to side effects:
- Metformin (patient unable to tolerate the nausea and vomiting);
- Vitamin B complex (caused drowsiness and vomiting);
- Perindopril (caused dizziness);
- Fluoxetine (caused insomnia).
In all instances, pharmacists communicated suggestions for alternative medicines to the doctors. In addition, SC patients reported hypoglycaemia-like symptoms (e.g. feeling dizzy, chills, sweating or experiencing headaches). A total of 23 episodes were recorded among 12.7% of patients (n=7) during the six-month period. Pharmacists educated patients on the prevention and management of hypoglycaemia.
The second most common MRP was sub-therapeutic dose (21.6%; n=65/301), followed by the need for additional therapy (17.3%; n=52/301). Medicine mainly related to sub-therapeutic doses of insulin were consequently solved by dose titration to achieve patient-individualised blood glucose targets. Pharmacists’ recommendations to add medicines included initiation of metformin, ACE-I/ARB, statin and aspirin.
However, not all pharmacist recommendations were accepted by the prescriber. There were 166 MRPs besides the identified non-adherence issues, such as unnecessary drug therapy, adverse drug reaction and the patient needing an additional drug. Pharmacists documented 30.7% (n=51) of interventions that were made in collaboration with doctors to achieve treatment goals. Of the 135 non-adherence problems, 44.4% (n=60) of interventions were made in collaboration with patients to increase adherence. Therefore, of the total 301 MRPs recorded, pharmacists documented 36.9% (n=111) interventions made in collaboration with patients and doctors to resolve the MRPs.
The most common interventions provided by pharmacists to improve adherence among SC patients were recommendations to buy a pill reminder device or providing a medicine timing chart (65.0%; n=39/60), followed by reinitiating drug therapy based on patient collaboration (35.0%; n=21/60). Table 4 presents the types of MRP identified, the causes of non-adherence, the list of pharmacists’ recommendations to prescribers and those accepted.
Table 4: Frequency of medicine– related problems identified by pharmacists for patients in the Simpler care arm over six months | |
| Medicine-related problems | Frequency (%) |
| Unnecessary drug therapy | 10 (3.3) |
| Needs additional drug therapy | 52 (17.3) |
| Ineffective drug | 29 (9.6) |
| Sub-therapeutic dose | 65 (21.6) |
| Adverse drug reaction | 4 (1.3) |
| Dosage too high | 6 (2.0) |
| Non-adherence | 135 (44.9) |
| Total | 301 (100) |
| Causes of non-adherence | Frequency (%) |
| Does not understand instructions | 14 (7.7) |
| Patient prefers not to take | 42 (23.1) |
| Patient forgets to take | 124 (68.1) |
| Cannot swallow or administer drugs | 2 (1.1) |
| Total | 182 (100) |
| Collaboration with patient | Frequency (%) |
| Reinitiated drug therapy in patients | 21 (35.0) |
| Pill reminder chart or device for patients | 39 (65.0) |
| Total | 60 (100) |
| Collaboration with doctor | Frequency (%) |
| Changed drug product | 6 (11.8) |
| Discontinued drug therapy | 5 (9.8) |
| Changed dosage | 17 (33.3) |
| Added additional medicine | 23 (45.1) |
| Total | 51 (100) |
The most common suggestion accepted by doctors, and consequent therapy change, was adding a medicine. This occurred in 45.1% (n=23/51) of doctor collaborations, followed by a dosage change, which occurred in 33.3% of patients (n=17/51). However, there was a non-significant difference between the number of patients prescribed medicines at six months compared to baseline between the two arms. Consequently, patient self-reported medicine adherence improved at six months compared with baseline. More patients reported never forgetting to take their medicines at six months (89.1%; n=49) compared with baseline (63.6%; n=35). Patients’ self-reported responses using a validated medicine compliance questionnaire (MCQ) are shown in Table 5, using four questions from the questionnaire[18]
.
Table 5: Medication adherence questionnaire results for the Simpler care arm | |||
| No. | Question | Baseline (n=55) |
Six months (n=55)
|
| Never (%) | Never (%) | ||
| 1. | How often do you forget to take your medicine? | 35 (63.6) | 49 (89.1) |
| 2. | How often do you miss taking your medicine because you feel better? | 47 (85.5) | 54 (98.2) |
| 3. | How often do you stop taking your medicine because you feel sick owing to effects of the medicine? | 46 (83.6) | 53 (96.4) |
| 4. | How often do you forget to bring along your medicine when you travel way from home? | 38 (69.1) | 50 (90.9) |
Lifestyle and patient education
Other interventions for non-adherence were focused on patient education and counselling to improve medicine adherence. All patients in the SC arm were educated on self-care management and lifestyle modifications during each visit. The types of education given followed the indicators in the Simpler tool (see Table 1). SC patients’ body mass index (BMI; P=0.481) and waist circumference (P =0.249) showed non-significant lower values, compared to UC patients. The duration of self-reported exercise increased at six months (57.4 minutes per week; SD=77.3) compared to baseline (35.8 minutes per week; SD=56.5) among the SC arm, and this increase was statistically significant (P=0.041).
Quality of life outcomes
The overall WHOQOL-BREF score improved significantly (P =0.007) in both arms at six months (note that a higher WHOQOL-BREF score denotes higher QOL)[16]
. The SC arm had significant improvements at all four domains at six months compared with baseline: physical health (P =0.002); psychological (P =0.042); social relationships (P =0.031); and environment (P =<0.001).
Two domains were significantly improved in the SC arm compared with the UC arm at six months: physical health (14.68 [SD=2.31] versus 13.70 [SD=2.30]; P=0.021); and environment (15.37[SD=2.16] versus 14.53 [SD=2.05]; P=0.030). Physical health incorporates activities of daily living, mobility and work capacity, while environment includes financial resources, home environment, health and social care, and opportunities for acquiring new information and skills.
The remaining two domains, namely psychological (e.g. bodily image and appearance, self-esteem, spirituality, negative and positive feelings, thinking, learning, memory and concentration) and social relationship (e.g. personal relationships, social support, sexual activity) showed no significant improvement between the arms. Table 6 compares the summary statistics for the WHOQOL-BREF scores converted to scores between 4–20, which is comparable with the WHOQOL-100[12]
.

Table 6. Changes in WHOQOL-BREF domain scores between both arms from baseline to six months follow-up (scores transformed from 4–20 according to WHOQOL-BREF manual)[12]
Discussion
The Simpler tool was successfully used in seven primary healthcare clinics in six districts in the state of Johor, Malaysia. Pharmacists without formal diabetes training applied the tool and identified medicine-related problems among SC patients. They made interventions that improved medicine adherence and QOL outcomes. Pharmacists also educated patients on lifestyle, medication management and cardiovascular risk reduction strategies that further contributed to patients’ overall improvements.
In this trial, pharmacists without formal diabetes training were purposively recruited. The findings demonstrated that pharmacists with limited clinical experience, but with adequate support through the Simpler intervention tool, effectively made medication interventions and improved QOL of T2DM patients in primary healthcare clinics in Malaysia. This suggests that there is scope to use the Simpler tool to train and support pharmacists with no formal T2DM management training.
The improved adherence scores of the SC patients at six months may be owing to increased patient education on knowledge and understanding of their medicine, which resulted in better self-management. This finding is consistent with two recent studies conducted in Malaysia and another study conducted in Hong Kong[20],[21],[22]
. In this study, the main cause of self-reported non-adherence was that patients forgot to take the medicine (68.1%; n=124). Most patients were on a minimum of four different medicines, namely metformin, ACEI, calcium channel blocker and simvastatin. Additionally, 21.8% (n=12) of patients had more than two comorbidities, which further increased the complexity of their medication regimen. This view is supported by a recent review, which found that medication regimen complexity was related to medication non-adherence[23]
.
In this study, ‘sub-therapeutic dose’ and ‘need addition of drugs’ were the most frequent medicine-related problems encountered. Pharmacists managed sub-therapeutic dose problems by suggesting dose optimisation specifically for metformin, perindopril and insulin. Pharmacists also collaborated with doctors to initiate medicines, such as ACEIs, insulin, metformin and statins. This is similar to a retrospective study involving multiple clinics in Malaysia where half of pharmacist interventions involved dosage adjustments and the remainder were changes to oral hypoglycaemic, cholesterol and antihypertensive medicines[24]
. Furthermore, pharmacists identifying medicine-related problems, such as adverse drug reactions, and solving these issues, may result in improved medication adherence as concluded in a 2004 study conducted among 2,985 patients in the United States[25]
.
Although the addition of insulin may be the cause of increased BMI, lifestyle interventions (e.g. diet and physical exercise) aimed to reduce patients’ weight problems. Nevertheless, the non-significant reduction in BMI and waist circumference among SC patients compared to UC patients at six months is consistent with several published RCTs conducted in Malaysia, the UK, United States, Hong Kong, Iran, Jordan, Australia and Brazil[22],[26],[27],[28],[29],[30],[31],[32]
. Similar to this study, an interdisciplinary approach involving multiple healthcare professional groups, such as nutritionists and physiotherapists, is lacking, highlighting a need for future studies following a multi-professional approach. Alternatively, a paid nutritional service that delivers nutritionally balanced meals and slimming centres that focus on technology may assist patients to achieve their BMI and waist circumference target. However, the cost of using these services may pose a barrier to some patients.
Previous studies have reported that uptake of physical exercise may be difficult among older and obese patients, which constituted the majority of this study population[33]
. Furthermore, exercising in hot and humid conditions can exert physiological strain, as shown in a previous study[34]
. Therefore, exercise may be more difficult to implement in a tropical climate where patients have little air conditioning or no access to air-conditioned gymnasiums.
Pharmacists who participated in this study received training in diabetes management and how to facilitate discussions with patients[11]
. SC patients were given education on diabetes self-management and on medication knowledge during their multiple visits to the pharmacist, and this may have improved medicine adherence. Another Malaysian study found that patient exposure to diabetes education increased medicine adherence and, subsequently, improved glycaemic control[20]
. In this study, education provided by pharmacists was culturally and religiously sensitive. Each pharmacist could converse in a minimum of two and up to four different languages, which further enhanced patient–pharmacist relationships. This is consistent with studies worldwide that have evaluated culturally sensitive educational programmes[35],[36]
. Pharmacists’ patient education on the beneficial effects of insulin in glycaemia control contributed to the overall improvement in HbA1c. This is consistent with a Malaysian qualitative study that reported lack of diabetes knowledge as the biggest barrier in achieving therapeutic targets[37]
.
Baseline QOL scores were statistically similar among both arms, suggesting that the baseline characteristics were homogenous. However, at six months, all single domains (physical health, psychological wellbeing, social relationships and environment) improved significantly in the intervention arm compared with baseline values. This was not the case for the control arm. The improvement in the single domains reflects the patients’ management of their daily tasks and could possibly be attributed to compliance to pharmacists’ lifestyle advice, as was suggested in a similar RCT[38]
. The two domains that showed significantly improved scores at six months comparing the intervention arm with the control arm were physical health and environment. The reason for the improved physical domain could be a result of increased daily activities, while the reason for improved scores on the environment domain could be owing to patients’ increased knowledge on diabetes self-management.
These findings are compatible with QOL results from a specific educational intervention conducted among diabetes patients in a diabetes clinic in Iran[39]
. Similar to our results, there were significant improvements in self-evaluation of QOL, self-assessment of health and the physical health domain comparing the intervention arm with the control arm[39]
. The findings of this study are also consistent with pharmacist-led diabetes intervention studies conducted in hospitals in Nigeria and India[38],[40]
and supports the conclusions of a pharmacist education intervention study conducted among outpatients in a medical centre in Malaysia[41]
.
The psychological domain in this study did not show significant improvement between the two arms. One reason could be attributed to the non-significant reduction in weight loss (BMI) for both arms, which is associated with body image. This view is consistent with a systematic review conducted on 36 studies that found improved body image was associated with weight loss[42]
. Body image is a facet relating to the psychological domain of the WHOQOL-BREF questionnaire. In addition, previous studies have found that weight loss led to improved mood and self-confidence, although it is acknowledged that there are multiple factors besides weight loss associated with mental health in diabetes[43]
.
Likewise, there was no significant improvement between groups for the social relationships domain. However, this domain was ranked the highest at baseline and at six months compared to the other three domains for both arms in this research. Similar high scores were found in a 2015 cross-sectional study conducted among T2DM patients from primary healthcare clinics in Malaysia, and in a 2016 study in Iran[44],[45]
. Correspondingly, the high social relationship domain scores could be attributed to the existing strong social support through individual, community and healthcare in Malaysia, as reported in a Malaysian study conducted among 175 patients in a primary care centre[46]
. Social support was considered important as it decreases diabetes distress and, subsequently, leads to improved outcomes, as documented in a systematic review of 30 studies[47]
. Nevertheless, in contrast to the UC patients, the SC patients had significant improvement pre- and post-intervention for this domain.
Limitations
In this RCT, both arms had the same number of follow-up visits. SC received care from intervention pharmacists using the Simpler tool, and the UC arm received monthly medicines and counselling if needed from the dispensing pharmacists. However, the patients in the SC arm had longer consultations with healthcare professionals. This could have contributed to the positive results as shown in some studies[48],[49]
Nevertheless, the methodology in this study is similar to previously published RCT studies where intervention patients had longer consultations[9]
.
This study produced different clinical outcomes. Certain information, such as medication lists for both intervention and control arms, were missing for some patients during the research period. Pharmacists were therefore contacted to retrieve the majority of the missing data. Other times, pharmacists had to contact patients to retrieve information, such as level of education and occupational background. The study period was only for six months, which is a relatively short period. Previous long-term studies have shown that patient improvement weaned after six months[41]
. Therefore, future studies should examine strategies to sustain patient improvements after the RCT study has ended or require long-term studies.
Medicine adherence, physical exercise duration and QOL evaluation relied on patients’ self-reported assessment. Previous studies have reported that patients tend to overrate their adherence to provide socially acceptable answers[50]
. In this study, pharmacists were required to follow up with patients every month for six months. However, it proved to be challenging as more than half of the patients recruited missed appointments or visited the pharmacy when pharmacists were busy with dispensing tasks and could not provide detailed care. Therefore, only 44.2% (n=34/77) of patients recruited managed to complete all six visits. Pharmacists’ efforts to remind patients of their appointments placed extra burden on their increasing workload. As a result, future research exploring digital platforms, such as mobile applications, telehealth or virtual visits, should focus on optimum intervals between patients and pharmacists to improve diabetes end points while still allowing room for self-care management.
Practice implications
Pharmacists, as part of a collaborative team, can use the Simpler tool to guide their interventions and provide education to enhance patient self-care management. This study used the Framingham risk score (see Table 1) to calculate cardiovascular disease risk, but this can be easily replaced with an appropriate risk prediction tool validated in the specific setting. Furthermore, the tool’s therapeutic targets were intended for Malaysian patients, but can be modified for use with a country’s specific practice guidelines.
Conclusion
Pharmacists successfully used the Simpler tool to make interventions that improved medicine adherence and QOL. Pharmacists also educated patients on lifestyle, medication management and cardiovascular risk reduction strategies, which further contributed to patients’ overall improvements. With the increasing prevalence of T2DM worldwide, a new notion for its management needs to be developed and this study has demonstrated that pharmacists using a structured, multifaceted diabetes intervention tool on seven targeted areas of care can achieve positive patient outcomes in overall disease management.
Acknowledgements
The authors would like to thank the director general of health for Malaysia for his permission to publish this article.
The authors would like to acknowledge the effort, dedication and contribution of all 14 participating pharmacists: Norain Mohd Puat, Christina Chan Yuin Theng, Nur Elyana Yazmin Mohd Redhuan, Lee Kok Pun, Nurul Huda Yasim, Ng Chen Kun, Nurul Azwa Ishak, Sharon Augustine Amburose, Nur Salwa Abdul Halim, Tan Hui Yng, Tey Sin Wei, Tan Cha Sin, Foong Yoke Kuan and Mohd Azmer Lias.
The authors would also like to thank Rosidah Md Din and Li Yun Chong for their support in this research.
Financial and conflicts of interest disclosure
This research did not receive any specific grant from funding agencies in the public, commercial or not-for-profit sectors. All authors have no financial disclosures or conflicts. All authors approved the final manuscript.
References
[1] World Health Organization. Global health estimates 2016: deaths by cause, age, sex, by country and by region, 2000–2016. 2018. Available at: https://www.who.int/healthinfo/global_burden_disease/estimates/en/index1.html (accessed August 2020)
[2] Mafauzy M, Zanariah H, Nazeri A & Chan SP. Diabcare 2013: a cross-sectional study of hospital based diabetes care delivery and prevention of diabetes related complications in Malaysia. Med J Malaysia 2016;71(4):177–185. PMID: 27770116
[3] Institute for Public Health. National health & morbidity survey 2015: non-communicable diseases, risk factors & other health problems. 2015. Available at: https://www.moh.gov.my/moh/resources/nhmsreport2015vol2.pdf (accessed August 2020)
[4] American Diabetes Association. Standards of medical care in diabetes. Diabetes Care 2016;39(S1). Available at: http://care.diabetesjournals.org/content/suppl/2015/12/21/39.Supplement_1.DC2/2016-Standards-of-Care.pdf (accessed August 2020)
[5] International Diabetes Federation. Global guideline for type 2 diabetes. 2012. Available at: https://www.iapb.org/wp-content/uploads/Global-Guideline-for-Type-2-Diabetes-IDF-2012.pdf (accessed August 2020)
[6] Ministry of Health Malaysia. Clinical practice guidelines. Management of type 2 diabetes mellitus. 2015. Available at: https://www.moh.gov.my/index.php/pages/view/134?mid=66 (accessed August 2020)
[7] National Institute for Health and Care Excellence. Type 2 diabetes in adults: management. NICE guideline [NG28]. 2019. Available at: https://www.nice.org.uk/guidance/ng28 (accessed: August 2020)
[8] Royal Australian College of General Practitioners. General practice management of type 2 diabetes 2016–18. 2016. Available at: https://www.racgp.org.au/FSDEDEV/media/documents/Clinical%20Resources/Guidelines/Diabetes/General-practice-management-of-type-2-diabetes_1.pdf (accessed August 2020)
[9] Ayadurai S, Hattingh HL, Tee LBG & Md Said SN. A narrative review of diabetes intervention studies to explore diabetes care opportunities for pharmacists. J Diabetes Res 2016. doi: 10.1155/2016/5897452
[10] Ayadurai S, Sunderland VB, Tee LBG & Hattingh HL. Consensus validation of Simpler: a tool to improve pharmacist delivery of quality, evidence-based diabetes care. Curr Diabetes Rev 2018;14(6):565–575. doi: 10.2174/1573399814666171215115239
[11] Ayadurai S, Sunderland B, Tee LB & Hattingh HL. A training program incorporating a diabetes tool to facilitate delivery of quality diabetes care by community pharmacists in Malaysia and Australia. Pharm Pract 2019;17(2):1457. doi: 10.18549/PharmPract.2019.2.1457
[12] World Health Organization. WHOQOL user manual, 2012 revision. 2012. Available at: https://apps.who.int/iris/handle/10665/77932 (accessed: August 2020)
[13] Trikkalinou A, Papazafiropoulou AK & Melidonis A. Type 2 diabetes and quality of life. World J Diabetes 2017;8(4):120–129. doi: 10.4239/wjd.v8.i4.120
[14] Wang H-f & Yeh MC. The quality of life of adults with type 2 diabetes in a hospital care clinic in Taiwan. Qual Life Res 2013;22:577–584. doi: 10.1007/s11136-012-0178-7
[15] Ayadurai S, Sunderland VB, Tee LBG et al. Structured tool to improve clinical outcomes of type 2 diabetes mellitus patients: a randomized controlled trial. J Diabetes 2018;10(12):965–976. doi: 10.1111/1753-0407.12799
[16] Hasanah CI, Naing L & Rahman AR. World Health Organization quality of life assessment: brief version in Bahasa Malaysia. Med J Malaysia 2003;58(1):79–88. PMID: 14556329
[17] Singhal PK, Raisch DW & Gupchup GV. The impact of pharmaceutical services in community and ambulatory care settings: evidence and recommendations for future research. Ann Pharmacother 1999;33(12):1336–1355. doi: 10.1345/aph.18440
[18] Ahmad NS, Ramli A, Islahudin F & Paraidathathu T. Medication adherence in patients with type 2 diabetes mellitus treated at primary health clinics in Malaysia. Patient Prefer Adherence 2013;7:525–530. doi: 10.2147/ppa.s44698
[19] Framingham Heart Study. Cardiovascular disease (10 year risk). 2018. Available at: https://www.framinghamheartstudy.org/risk-functions/cardiovascular-disease (accessed August 2020)
[20] Al-Qazaz HK, Sulaiman SA, Hassali MA et al. Diabetes knowledge, medication adherence and glycemic control among patients with type 2 diabetes. Int J Clin Pharm 2011;33:1028–1035. doi: 10.1007/s11096-011-9582-2
[21] Chow EP, Hassali MA, Saleem F & Aljadhey H. Effects of pharmacist-led patient education on diabetes-related knowledge and medication adherence: a home-based study. Health Educ J 2016;75(4):421–433. doi: 10.1177/0017896915597021
[22] Chan CW, Siu SC, Wong CKW & Lee VWY. A pharmacist care program: positive impact on cardiac risk in patients with type 2 diabetes. J Cardiovasc Pharmacol Ther 2012;17(1):57–64. doi: 10.1177/1074248410396216
[23] Wimmer BC, Cross AJ, Jokanovic N et al. Clinical outcomes associated with medication regimen complexity in older people: a systematic review. J Am Geriatr Soc 2017;65(4):747–753. doi: 10.1111/jgs.14682
[24] Lee XY, Selvadurai S, Cheah Ky et al. Impact of pharmacist-managed diabetes medication therapy adherence clinic (DMTAC) in government health clinics. Malaysian Journal of Pharmaceutical Sciences 2015;13(1):43–51. Available at: http://mymedr.afpm.org.my/publications/46168 (accessed August 2020)
[25] Strand LM, Cipolle RJ, Morley PC & Frakes MJ. The impact of pharmaceutical care practice on the practitioner and the patient in the ambulatory practice setting: twenty-five years of experience. Curr Pharm Des 2004;10(31):3987–4001. doi: 10.2174/1381612043382576 (accessed August 2020)
[26] Jameson JP & Baty PJ. Pharmacist collaborative management of poorly controlled diabetes mellitus: a randomized controlled trial. Am J Manag Care 2010;16(4):250–255. PMID: 20394460
[27] Taveira TH, Friedmann PD, Cohen LB et al. Pharmacist-led group medical appointment model in type 2 diabetes. Diabetes Educ 2010;36(1):109–117. doi: 10.1177/0145721709352383
[28] Farsaei S, Sabzghabaee AM, Zargarzadeh AH & Amini M. Effect of pharmacist-led patient education on glycemic control of type 2 diabetics: a randomized controlled trial. J Res Med Sci 2011;16(1):43–49. PMID: 21448382
[29] Mehuys E, Van Bortel L, De Bolle L et al. Effectiveness of a community pharmacist intervention in diabetes care: a randomized controlled trial. J Clin Pharm Ther 2011;36(5):602–613. doi: 10.1111/j.1365-2710.2010.01218.x
[30] Jarab AS, Alqudah SG, Mukattash TL et al. Randomized controlled trial of clinical pharmacy management of patients with type 2 diabetes in an outpatient diabetes clinic in Jordan. J Manag Care Pharm 2012;18(7):516–526. doi: 10.18553/jmcp.2012.18.7.516
[31] Magalhães AOM, Ferreira WR, Martins MAP et al. Pharmaceutical care program for type 2 diabetes patients in Brazil: a randomised controlled trial. Int J Clin Pharm 2013;35(1):79–86. doi: 10.1007/s11096-012-9710-7
[32] Chua SS, Kok LC, Yusof FA et al. Pharmaceutical care issues identified by pharmacists in patients with diabetes, hypertension or hyperlipidaemia in primary care settings. BMC Health Serv Res 2012;12(1):1–10. doi: 10.1186/1472-6963-12-388
[33] Willey KA & Singh MA. Battling insulin resistance in elderly obese people with type 2 diabetes: bring on the heavy weights. Diabetes Care 2003;26(5):1580–1588. doi: 10.2337/diacare.26.5.1580
[34] Hue O. The challenge of performing aerobic exercise in tropical environments: applied knowledge and perspectives. Int J Sports Physiol Perform 2011;6(4):443–454. doi: 10.1123/ijspp.6.4.443
[35] Mohamed H, Al-Lenjawi B, Amuna P et al. Culturally sensitive patient-centred educational programme for self-management of type 2 diabetes: a randomized controlled trial. Prim Care Diabetes 2013;7(3):199–206. doi: 10.1016/j.pcd.2013.05.002
[36] DePue J, Dunsiger S, Seiden A et al. Nurse-community health worker team improves diabetes care in American Samoa: results of a randomized controlled trial. Diabetes Care 2013;36(7):1947–1953. doi: 10.2337/dc12-1969
[37] Ali S & Jusoff K. Barriers to optimal control of type 2 diabetes in Malaysian Malay patients. Glob J Health Sci 2009;1(2):106–118. doi: 10.5539/gjhs.v1n2p106
[38] Adibe MO, Ukwe CV & Aguwa CN. The impact of pharmaceutical care intervention on the quality of life of Nigerian patients receiving treatment for type 2 diabetes. Value Health Reg Issues 2013;2(2):240–247. doi: 10.1016/j.vhri.2013.06.007
[39] Taghdisi MH, Borhani M, Solhi M et al. The effect of an education program utilising PRECEDE model on the quality of life in patients with type 2 diabetes. Health Educ J 2012;71(2):229–238. doi: 10.1177/0017896911398812
[40] Ramanath KV, Bhanuprakash M, Nagakishore CHet al. Study the clinical phamacist influence on medication adherence & quality of life of rural type-2 diabetes mellitus patients in a tertiary care hospital. Arch Pharm Pract 2012;3(2):170–180. Available at: https://archivepp.com/en/article/study-the-clinical-phamacist-influence-on-medication-adherence-quality-of-life-of-rural-type-2-diabetes-mellitus-patients-in-a-tertiary-care-hospital (accessed August 2020)
[41] Butt M, Ali AM, Bakry MM & Mustafa N. Impact of a pharmacist led diabetes mellitus intervention on HbA1c, medication adherence and quality of life: a randomised controlled study. Saudi Pharm J 2016;24(1):40–48. doi: 10.1016/j.jsps.2015.02.023
[42] Lasikiewicz N, Myrissa K, Hoyland A & Lawton CL. Psychological benefits of weight loss following behavioural and/or dietary weight loss interventions. A systematic research review. Appetite 2014;72:123–137. doi: 10.1016/j.appet.2013.09.017
[43] Miller-Kovach K, Winick M & Hermann M. The psychological ramifications of weight management. J Womens Health Gend Based Med 1999;8(4):477–482. doi: 10.1089/jwh.1.1999.8.477
[44] Chew B-h, Mohd-Sidik S & Shariff-Ghazali S. Negative effects of diabetes-related distress on health-related quality of life: an evaluation among the adult patients with type 2 diabetes mellitus in three primary healthcare clinics in Malaysia. Health Qual Life Outcomes 2015;13. doi: 10.1186/s12955-015-0384-4
[45] Didarloo A & Alizadeh M. Health-related quality of life and its determinants among women with diabetes mellitus: a cross-sectional analysis. Nurs Midwifery Stud 2016;5(1):e28937. PMID: 27331054
[46] Chew BH, Khoo EM & Chia YC. Social support and glycemic control in adult patients with type 2 diabetes mellitus. Asia Pac J Public Health 2015;27(2):166–173. doi: 10.1177/1010539511431300
[47] Rosland A-m, Heisler M & Piette JD. The impact of family behaviors and communication patterns on chronic illness outcomes: a systematic review.J Behav Med 2012;35(2):221–239. doi: 10.1007/s10865-011-9354-4
[48] Mshelia DS, Akinosun OM & Abbiyesuku FM. Effect of increased patient-physician contact time and health education in achieving diabetes mellitus management objectives in a resource-poor environment. Singapore Med J 2007;48(1):74–79. PMID: 17245520
[49] Swinnen SGHA & DeVries JH. Contact frequency determines outcome of basal insulin initiation trials in type 2 diabetes. Diabetologia 2009;52:2324–2327. doi: 10.1007/s00125-009-1527-0
[50] Osterberg L & Blaschke T. Adherence to medication. N Engl J Med 2005;353:487–497. doi: 10.1056/NEJMra050100


