Shutterstock.com
After reading this article, you should be able to:
- Describe the major types and underlying pathophysiology of aortic diseases, including aortic aneurysms and dissections, and understand their clinical significance;
- Recognise the clinical presentation and diagnostic workup of acute aortic syndromes, including typical and atypical symptoms, imaging modalities and relevant biomarkers;
- Outline current management approaches for aortic disease, including medical therapy, especially in patients with Marfan syndrome, and their role in slowing disease progression.
Introduction
Aortic dissection (i.e. tearing of the aorta) and aortic aneurysms (i.e. swelling of the aorta) are considered severe types of aortic disease. They are potentially life threatening if not treated within a timely manner. These disorders often present late with acute symptoms and require prompt diagnosis and management to prevent severe complications, such as rupture, organ ischaemia or death1.
There are approximately 5,000 deaths each year in the UK owing to ruptured aortic aneurysms. Aortic dissection and aortic aneurysms are most common in men aged 65 years and older, accounting for around 1 in 75 deaths within this age group1.
Pharmacists play a pivotal role in the multidisciplinary approach to aortic disease care. By conducting thorough medication reviews and optimising cardiovascular disease (CVD) risk factor control — such as managing hypertension, dyslipidaemia, diabetes and smoking cessation — pharmacists can help slow disease progression and prevent acute aortic events. Expertise in pharmacotherapy ensures appropriate use of antihypertensives (e.g., beta-blockers, ACE inhibitors), lipid-lowering agents and antiplatelet therapies when indicated — all of which contribute to reducing aortic wall stress and enhancing vascular health.
Pharmacists in both primary and secondary care settings are well-positioned to identify at-risk patients (e.g. those with Marfan syndrome, a family history of aortic disease or uncontrolled blood pressure) and prompt timely referrals for imaging and specialist evaluation. With growing involvement in chronic disease management and patient education, pharmacists are integral to improving outcomes in aortic disease through preventive strategies and interdisciplinary care coordination.
Pathophysiology
The aorta is the body’s main blood vessel. Over a person’s lifetime, it carries around 200 million litres of blood from the heart to the rest of the body2. The aorta is divided into two main parts by the diaphragm: the thoracic aorta and the abdominal aorta. The wall of the aorta has three layers:
- The inner layer (i.e. tunica intima), which is thin and lined with cells called endothelium;
- The middle layer (i.e. tunica media), which is much thicker and contains elastic tissue and smooth muscle, helping the aorta stretch and contract with each heartbeat;
- The outer layer (i.e. tunica adventitia), which is made mostly of collagen and contains small blood vessels and lymphatic vessels that help nourish the wall of the aorta2.
The aorta plays an important role in the control of systemic vascular resistance and heart rate, via pressure–responsive receptors located in the ascending aorta and aortic arch. An increase in aortic pressure results in a decrease in heart rate and systemic vascular resistance, whereas a decrease in aortic pressure results in an increase in heart rate and systemic vascular resistance2.
Figure 1: The anatomical divisions of the aorta
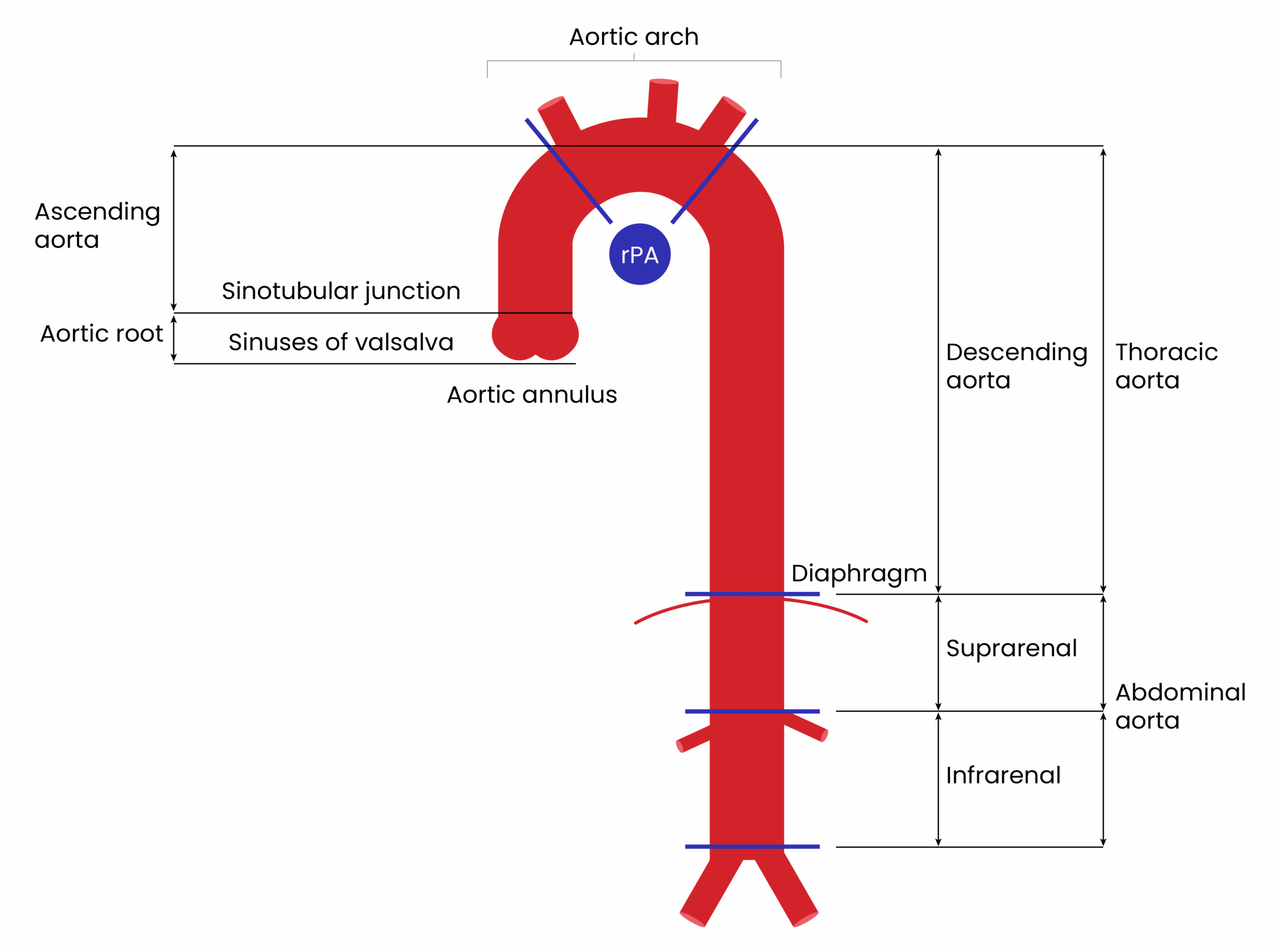
Adapted from EHJ, 2014
In healthy adults, aortic diameters do not usually exceed 40mm and taper gradually downstream2. The variability is influenced by several factors, including age, gender, body size and blood pressure. The rate of aortic expansion is about 0.9mm in men and 0.7mm in women for each decade of life2. This slow but progressive aortic dilation over mid-to-late adulthood is thought to be a consequence of ageing, which is related to a higher collagen-to-elastin ratio, along with increased stiffness and pulse pressure2.
There is an association of genetic involvement to aortic diseases. Marfan syndrome is a systemic connective tissue disorder caused by mutations in the FBN1 gene, which encodes fibrillin-1 — a protein essential for the structural integrity of elastic fibres in connective tissue3. This autosomal-dominant condition presents with a wide range of clinical manifestations, affecting the skeletal, ocular and cardiovascular systems3. Characteristics of individuals with Marfan syndrome include tall height and long and slender limbs. Cardiovascular complications are the most life-threatening manifestations, with the most serious concern being progressive aortic root dilation and the potential for aortic aneurysm and dissection3.
The aorta in individuals with Marfan syndrome is structurally weakened, owing to abnormal fibrillin-1, predisposing it to abnormal dilation and rupture3. Without timely diagnosis and intervention, aortic dissection — particularly of the ascending aorta — can occur, often with catastrophic outcomes3. Understanding the natural history, risk factors and management strategies of aortic disease in Marfan syndrome is crucial for improving patient outcomes and preventing sudden cardiac death.
Aortic aneurysm
An aortic aneurysm is a condition that is defined as a permanent, localised dilation of the aorta to a diameter >50% greater than normally expected2. This condition can affect any segment of the aorta, as outlined in Figure 1, which could include the ascending aorta, aortic arch, descending thoracic or abdominal segments2. Table 1 summarises the different types of aortic aneurysms based on anatomical location3.
Table 1: The different types of aortic aneurysms based on anatomical location
Most patients are asymptomatic, and the condition can remain undetected until complications arise. European Society of Cardiology (ESC) guidelines highlight that the classic presentation of a ruptured abdominal aortic aneurysm (AAA) includes abdominal pain, hypotension and a pulsatile abdominal mass, which may be present with abdominal or back pain2. Since the clinical presentation of ruptured AAA may mimic other abdominal emergencies, early recognition is important. For thoracic aortic aneurysm (TAA), symptoms may include chest or back pain, hoarseness or dysphagia, depending on the location. However, many patients remain asymptomatic until the aneurysm reaches a critical size or ruptures2.
Aortic dissection
Aortic dissection is a life-threatening condition, characterised by the formation of a false lumen within the aortic wall owing to a tear in the intima, which allows blood to flow between the layers of the aortic wall2,4. This separation can lead to compromised blood flow to vital organs and is associated with high mortality, if not promptly diagnosed and treated. The risk of death increases by 1–2% per hour in the first 24–48 hours for type A dissection for each hour that passes without treatment5.
Patients with aortic dissection often present with sudden onset, severe chest or back pain, which is described as sharp, tearing or ripping4. Other symptoms may include syncope and neurological deficits, depending on the location and extent of dissection4.
ESC guidelines primarily utilise the Stanford classification to categorize aortic dissections:
- Type A: Involves the ascending aorta and may extend to the aortic arch and descending aorta. This type requires urgent surgical intervention due to the risk of complications such as rupture, pericardial tamponade (compression of the heart due to accumulation of fluid in the pericardial sac) and aortic valve insufficiency2,4;
- Type B: Confined to the descending aorta distal to the left subclavian artery. Management is typically medical focusing on blood pressure control and pain relief2,4. Surgical or endovascular intervention is considered if complications like rupture, malperfusion or persistent pain occur2,4.
Risk factors
Understanding the risk factors associated with aortic disorders is essential for early detection, prevention and therapeutic intervention4.
Chronic hypertension is the most significant risk factor for both aortic aneurysms and aortic dissection2,4. Increased blood pressure contributes to the mechanical stress on the aortic wall, which over time leads to weakening, dilation and possible rupture or dissection2. The incidence of aortic dissection is particularly elevated in individuals with long-standing, uncontrolled hypertension2,4,6.
Age is a significant risk factor for aortic diseases. The prevalence of aortic aneurysms increases with age, particularly in individuals older than 65 years. The risk of aortic dissection also increases with age and commonly occurs in individuals aged 60–70 years. It is more common in males than females, with the male-to-female ratio in aortic dissection cases being approximately 2:12,4,6.
Certain genetic conditions predispose individuals to aortic diseases by affecting the integrity of the aortic wall2. Family history also plays a significant role, with first-degree relatives of individuals with aortic diseases having a higher risk2. As well as Marfan syndrome, Ehlers-Danlos syndrome is another connective tissue disorder that can lead to vascular fragility, increasing the risk of aneurysms and dissections2,6. Bicuspid aortic valve is a congenital condition associated with an increased risk of aortic aneurysms, particularly in the ascending aorta2. These patient groups are monitored regularly owing to their increased risk, usually by cardiac imaging such as an echocardiogram. The severity of their condition and age will determine the type of monitoring and frequency7.
Atherosclerosis, particularly when combined with smoking, is a major risk factor for aortic diseases1,2. The presence of atherosclerotic plaques in the aorta can weaken the vessel wall, making it more prone to aneurysmal dilation and dissection. Smoking accelerates the development of atherosclerosis and is particularly harmful in individuals predisposed to aortic aneurysms1,2.
Diagnosis
The diagnosis of suspected aortic disorders involves a complete physical examination, blood pressure and history from the patient but will also involve the following to aid diagnosis and management:
- Computed tomography angiography (CTA), which is usually first line owing to specificity and provides detailed images of the aorta;
- Electrocardiogram (ECG) to evaluate chest pain and rule out other conditions e.g. myocardial infarction;
- Chest x-ray, which is an indication of aortic dissection that may include a widened mediastinum, abdominal aortic contour or pleural effusion;
- Transthoracic/transoesophageal echocardiography provides fewer clear images but useful in diagnosing complications related to aortic dissection;
- Magnetic resonance imaging (MRI) provides clear images, useful in patients with allergies to iodine2.
Blood tests provide a variety of indicators that aid diagnosis and management of aortic disorders (see Table 26).
Clinical presentation of aortic aneurysm and dissection
Aortic aneurysms and dissections are life-threatening conditions that often present with non-specific symptoms, posing significant diagnostic challenges. Clinical pharmacists should be aware of their varying presentations to support prompt recognition and multidisciplinary management.
The symptoms of an aortic aneurysm vary depending on its anatomical location — abdominal or thoracic — and may remain asymptomatic until complications arise, such as rupture or dissection.
AAA
Patients with an AAA may be asymptomatic or present with non-specific symptoms. When symptomatic, common clinical features include2,6,8:
- A pulsatile abdominal mass;
- Abdominal or lower back pain;
- A sense of fullness or pressure in the abdomen;
- In some cases, pain may radiate to the groin, buttocks, or legs.
Rupture of an AAA is a medical emergency and can present with sudden, severe abdominal or back pain, hypotension and signs of cardiac shock.
TAA
Symptoms of thoracic aortic aneurysms depend on the size and location of the aneurysm. Many cases are asymptomatic and discovered incidentally. When present, symptoms may include2,6,8:
- Chest or upper back pain, which may mimic myocardial ischemia;
- Pain radiating to the neck, jaw or shoulders;
- Hoarseness owing to compression of the recurrent laryngeal nerve;
- Dysphagia from oesophageal compression;
- Cough or shortness of breath related to tracheal or bronchial compression;
- In some cases, symptoms may be owing to thromboembolism or aortic regurgitation.
Both AAA and TAA may present acutely if rupture or dissection occurs, which requires immediate emergency intervention. Symptoms that are experienced by patients are outlined above.
Management of aortic diseases
While not all patients with aortic disease require surgical intervention, medical therapy is essential in both acute and chronic settings to manage symptoms, maintain haemodynamic stability and reduce disease progression. A multidisciplinary, patient-centred approach, combining pharmacological and procedural options, is essential to optimising outcomes.
For all patients with aortic pathology, the following modifiable cardiovascular risk factors should be aggressively managed, in line with ESC recommendations:
- Systolic blood pressure should have a target of <130 mmHg;
- Serum LDL-C should have a target of <1.4 mmol/L;
- Smoking cessation is strongly advised in all cases2;
- Pharmacists are well placed to support patients with monitoring their blood pressure regularly, optimising antihypertensives and providing education on medication adherence and healthy lifestyle changes. For example, providing support to stop smoking, offering nicotine replacement therapies (e.g. nicotine patches, lozenges) and maintaining a healthy, balanced diet.
Management of aortic dissections
An overview of the management of aortic dissections can be seen in Figure 22.
Figure 2: Management of type A and type B aortic dissections
Management of aortic aneurysms
Aortic aneurysms can be managed medically; however, surgical repair is indicated in the following situations:
- Ascending aortic aneurysm: Surgical repair considered when the diameter exceeds 55 mm in men and 50 mm in women, or earlier if genetic disorders (e.g. Marfan syndrome) are present;
- Abdominal aortic aneurysm: Repair recommended at ≥55 mm for men, ≥50 mm for women, or if rapid expansion (>10 mm/year) is observed2.
Open surgical repair is a long-established option with durable outcomes2. Thoracic endovascular aortic repair (TEVAR) is preferred in older patients or those with significant comorbidities, with reduced perioperative risk2.
Medical therapy is critical both in the acute setting and long-term to stabilise the aneurysm and reduce rupture risk:
- Intravenous beta-blockers (e.g., labetalol or esmolol) to rapidly reduce shear stress in the acute period;
- RAAS inhibitors for long-term blood pressure control (e.g. Ramipril long term);
- Statin therapy to reduce vascular inflammation and aortic expansion (e.g. atorvastatin long term);
- Antiplatelet agents indicated in the presence of coexisting atherosclerotic disease (e.g. aspirin long term);
- Smoking cessation and lipid control remain central to risk mitigation.
Some complications, which can occur following aortic disease and surgical intervention, can include the following5:
- Cardiac tamponade (i.e. the compression of the heart owing to accumulation of fluid in the pericardial sac);
- Aortic incompetence or regurgitation (i.e. the aortic valve doesn’t close properly, causing a backflow of blood);
- Myocardial infarction (i.e. a sudden reduction of/or blockage of blood flow to the heart);
- Aneurysmal degeneration/rupture (i.e. a weakening of the artery wall/aorta, which can lead to a tear and severe bleeding);
- Regional ischaemia (i.e. reduced blood flow to a local area of tissue resulting in inadequate oxygen supply);
- Left arm ischaemia/subclavian steal syndrome, which is a condition that diverts blood flow away from the brain to the arm, owing to subclavian artery narrowing);
- Endovascular leaking (i.e. the leaking of blood outside a stent graft into an aneurysm sac)5.
Non-pharmacological management
Following aortic dissection, patients should be advised to avoid contact sports and strenuous physical activities (e.g. isometric heavy weightlifting, pushing or straining that would require a Valsalva manoeuvre (i.e. forced exhalation against a closed airway)) to reduce aortic wall shear stress owing to sudden rises in arterial blood pressure during exercise2,8,9. Aerobic exercise may be acceptable after careful consideration and discussion, ideally keeping the patient’s heart rate below 100 beats per minute2. A patient must be reviewed by a specialist before exercising to identify risks and to develop a safe and effective plan for physical activity10. Patients should follow up for surveillance imaging and blood pressure control2. Maintaining smoking cessation is also vital to reduce future risks.
Monitoring
It is crucial that imaging of the aorta is performed for patients before being discharged from hospital. This will aid with identifying any complications, such as aortic enlargement or rupture.
The time intervals recommended for surveillance imaging with computed tomography angiography (CTA) or magnetic resonance angiography in patients with chronic aortic dissection vary across guidelines and should be tailored for individual patients. Such guidelines include:
- NICE guideline ‘Abdominal aortic aneurysm: diagnosis and management’, published in 202010;
- The American College of Cardiology and American Heart Association guideline for the diagnosis and management of aortic disease, published in 202211;
- ESC guidelines for the management of peripheral arterial and aortic diseases, published in 202412.
The ESC guidance currently recommends12:
- Patients with uncomplicated aortic dissection who being medically managed should be followed up at six months post-diagnosis;
- Patients who have undergone TEVAR should be followed up with imaging at 1, 6, and 12 months postoperatively, and then annually thereafter. If an abnormality is detected, shorter intervals may be required;
- CTA is recommended as the imaging of choice for follow-up of patients who have undergone TEVAR; however, MRI is preferred in younger patients if they have magnetic-resonance compatible stent grafts, to reduce radiation exposure;
- Patients who have undergone open surgery can have follow-up at approximately five-year intervals with doppler ultrasound or CTA2.
Specific frequencies for reviewing medication also vary across guidelines; however, evaluations are recommended at 3, 6 and 12 months following aortic dissection and annually thereafter, with adjustments to antihypertensive therapies made as required to achieve a target of <130mmgHg for everyone.
Summary
Timely diagnosis and appropriate intervention are critical in the management of aortic diseases, such as aortic aneurysms and dissections, owing to their potential for rapid progression and high mortality if left untreated. Early detection significantly reduces the risk of life-threatening complications, including rupture, ischemia and death.
Further resources
- British Heart Foundation: All about aortic aneurysm;
- British Heart Foundation: Aortic aneurysm, dissection and rupture;
- European Society of Cardiology: ‘Guidelines for the management of peripheral arterial and aortic diseases’;
- NICE: ‘Abdominal aortic aneurysm: diagnosis and management’.
- 1.All about aortic aneurysm . British Heart Foundation. https://www.bhf.org.uk/informationsupport/heart-matters-magazine/medical/all-about-aortic-aneurysm
- 2.2014 ESC Guidelines on the diagnosis and treatment of aortic diseases. Eur Heart J. 2014;35(41):2873-2926. doi:10.1093/eurheartj/ehu281
- 3.AIMS trial – can we prevent heart complications in people with Marfan syndrome? British Heart Foundation. https://www.bhf.org.uk/what-we-do/our-research/impact-of-clinical-trials/aims-trial
- 4.Nienaber CA, Clough RE. Management of acute aortic dissection. The Lancet. 2015;385(9970):800-811. doi:10.1016/s0140-6736(14)61005-9
- 5.Elendu C, Amaechi DC, Elendu TC, Ibhiedu JO, Torubiri AO, Okoye OK. Comprehensive review of aortic aneurysms, dissections, and cardiovascular complications in connective tissue disorders. Medicine. 2023;102(48):e36499. doi:10.1097/md.0000000000036499
- 6.Clinical features and diagnosis of thoracic aortic aneurysm and dissection . UpToDate. https://www.uptodate.com/contents/clinical-features-and-diagnosis-of-acute-aortic-dissection
- 7.Regalado ES, Morris SA, Braverman AC, et al. Comparative Risks of Initial Aortic Events Associated With Genetic Thoracic Aortic Disease. Journal of the American College of Cardiology. 2022;80(9):857-869. doi:10.1016/j.jacc.2022.05.054
- 8.Hiratzka LF, Bakris GL, et al. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the Diagnosis and Management of Patients With Thoracic Aortic Disease. Circulation. 2010;121(13). doi:10.1161/cir.0b013e3181d4739e
- 9.Qazi M, Prakash S. Aortic diseases: tips for promoting medication and exercise compliance . Endovascular Today. 2024. https://evtoday.com/articles/2024-nov/aortic-diseases-tips-for-promoting-medication-and-exercise-compliance
- 10.Abdominal aortic aneurysm: diagnosis and management (NG156) . National Institute for Health and Care Excellence. March 2020. https://www.nice.org.uk/guidance/ng156
- 11.Isselbacher EM, Preventza O, Hamilton Black J III, et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2022;146(24). doi:10.1161/cir.0000000000001106
- 12.Mazzolai L, Teixido-Tura G, Lanzi S, et al. 2024 ESC Guidelines for the management of peripheral arterial and aortic diseases. European Heart Journal. 2024;45(36):3538-3700. doi:10.1093/eurheartj/ehae179
You might also be interested in…

NICE draft guidance recommends finerenone for type of chronic heart failure

Blood pressure and cholesterol in older adults with obesity found to be similar to people with healthy BMIs