

Victoria Sharratt / Shutterstock.com
After reading this article, you should be able to:
- Know common interactions with glucocorticoids and how these can be managed;
- Understand the differences between mineralocorticoid and glucocorticoid-related side effects and how they are managed;
- Provide appropriate vaccination advice for patients taking glucocorticoids;
- Know the different types of steroid card, when each is used and when sick day advice is required.
Introduction
Glucocorticoids (GC) are steroid hormones that have a significant role in regulating various physiological processes, including in metabolism and the body’s response to stress1. The potent anti-inflammatory effects of GC make this class of medication crucial in the management of various chronic inflammatory diseases2.
Synthetic GC have been used for decades in the treatment of chronic inflammatory conditions, with their use first documented in 1948 for the treatment of rheumatoid arthritis3. When used for long-term disease control, prednisolone is the most prescribed oral GC in the UK4. Asthma and chronic obstructive pulmonary disease (COPD) are the conditions most frequently treated with oral GC5.
While GC are highly effective at treating chronic inflammatory conditions, their use has significant short- and long-term risks5. In the short term, GC can increase the risk of infection and gastrointestinal ulceration, while long-term exposure is associated with complications, including osteoporosis, type 2 diabetes mellitus and cataracts. The likelihood of complications increases with both higher dosages and prolonged cumulative exposure. Furthermore, the risks of abrupt withdrawal of GC after prolonged exposure — even at low doses — can put patients at significant risk of adrenal insufficiency and adrenal crisis6.
As experts on medicines, pharmacists are well placed in both community and hospital settings, to provide counselling on the risks of oral GC to patients. This article will cover appropriate counselling for patients starting oral GC. It is most relevant to patients on long-term, high-dose oral GC but may apply to other patient groups, including those at increased risk of complications such as patients with diabetes.
Interactions
As with all newly started medications, a review of the patient’s current medications and clinical history should be completed prior to starting oral GCs. See Figure 1 for an overview of some drug interactions with GCs, but this list is not exhaustive7–14.
Figure 1: Drug interactions with oral GC including examples and management
Overview of side effects
GC do not often cause side effects if they are taken for a short period of time or at a low dose. For detail on what is considered high-dose or long-term GC, see Table 14,7. Prednisolone is used as an example of a widely used oral GC7. Side effects are dependent on the type, strength and treatment duration, and usually cease when treatment is complete15.
Table 1: Examples of high-dose, long-term oral prednisolone treatments
Excessive dosage or prolonged use of GC may potentiate their normal physiological effects, resulting in mineralocorticoid and glucocorticoid-related side effects (see Table 2)15,16. Mineralocorticoids manage fluid and electrolyte balance, while glucocorticoids regulate metabolism and stress response.
Patients should be advised to consult with their medical team if any of these side effects are experienced. Patients are at increased risk of developing infection while taking GC. It is important to rule out underlying infection prior to initiating therapies, patients should seek medical attention if they develop signs of infection. Hygiene practices should be encouraged including food and hand hygiene. See Table 2 for further information15–19.
Table 2: Common side effects associated with oral GC
General principles for managing side effects can be seen in Box 116,18.
Box 1: General principles for managing side effects
- To minimise glucocorticoids (GC) side effects, the lowest effective dose should be used for the minimum period possible;
- In some situations, the total dose for two days can sometimes be taken as a single dose on alternate days or by means of intermittent therapy with short courses;
- In some conditions, it may be possible to reduce the GC dose with the addition of an immunosuppressive drug (e.g. methotrexate) to achieve a ‘steroid-sparing effect’;
- Ensure patients carry a steroid emergency card, where applicable20,21;
- Any suspected side effects should be reported via the Medicines and Healthcare products Regulatory Agency’s Yellow Card scheme22.
Proton pump inhibitors as an adjunct to oral GC
Proton pump inhibitors (PPIs) can be prescribed alongside oral GC to reduce the risk of gastrointestinal ulcers7,8. Risk factors include patients with a history of gastrointestinal bleeding, perforation or ulceration or those taking medications that increase GI bleeding risk (e.g. non-steroidal anti-inflammatory drugs (NSAIDs)). PPIs should be considered in patients who are of older age, heavy smokers, who have excessive alcohol intake or have serious comorbidities such as advanced cancer7.
Serious side effects
Although rare, serious side effects can occur. There is a risk of risk of central serous chorioretinopathy (i.e. fluid leaking under the macula, causing vision disturbances), patients should be advised to report any vision problems or disturbances, especially affecting one eye rather than both. If a patient presents with vision problems, refer to an ophthalmologist for evaluation of possible causes or alternatively, advise the patient to attend their nearest eye casualty.
If a patient presents with symptoms of adrenal crisis (e.g. severe hypotension, dizziness, severe nausea/vomiting), they should be advised to attend an emergency department urgently. Adrenal crises can occur in patients on long-term GC owing to trauma, illness, surgery and severe emotional stress. It is an emergency requiring treatment with intravenous steroids and fluids, as well as possible intensive care admission23. When starting high-dose or long-term oral GC, patients should be counselled on the risks of adrenal insufficiency and adrenal crisis7. Patients and healthcare professionals should be aware of symptoms of adrenal crisis (e.g. nausea, vomiting, fatigue, fever, weight loss, anorexia, abdominal pain, hypotension, hyponatraemia, hyperkalaemia, hypoglycaemia) and what to do if these occur24.
Vaccinations
In some situations, live vaccines can cause severe or fatal infections in immunosuppressed individuals owing to extensive replication of the vaccine strain23. Live vaccines should not be given to patients (i.e. adults and children) receiving or who have in the past three months received:
- High-dose GC (i.e. >40mg prednisolone per day or 2mg/kg per day in children under 20kg) for more than one week;
- Lower-dose GC (i.e. >20mg prednisolone per day or 1mg/kg per day in children under 20kg) for more than two weeks.
Live vaccines may be given to immunosuppressed individuals if deemed appropriate according to Green Book guidance and their specialist (see Box 2)23.
Box 2: Current live vaccinations used in the UK
- Rotavirus;
- Yellow fever;
- Measles, mumps and rubella (Priorix, MMRVaxPro);
- Influenza (nasal) (Fluenz Tetra);
- Bacillus Calmette-Guérin;
- Varicella vaccine (Varilix, Varivax);
- Oral typhoid vaccine (Ty21a);
- Shingles vaccine (Zostavax).
As live vaccines replicate after administration, ideally individuals who have received a live vaccine should wait until their immune response has been established to receive immunosuppressive therapy7,23. For most viral live vaccines, a period of up to four weeks should be sufficient. However, as viruses in vaccines are generally attenuated, immunosuppressive treatment should not be delayed if this would result in the worsening of the underlying condition7,23. Patients and pharmacists should engage with the clinical team when live vaccination is considered for individuals undergoing immunosuppressive therapy.
Inactivated vaccines cannot be replicated and, therefore, may be administered to immunosuppressed individuals; although they may elicit a lower immune response7,23. Where possible, inactivated vaccines should be given at least two weeks before treatment; however, they may be given during treatment, if deemed necessary.
Considerations for bone health
GC are associated with an increased risk of bone loss, which is more pronounced in the first few months of use, as well as bone fracture, which can occur with prednisolone or its equivalent at doses as low as 2.5 to 7.5mg daily25,26.
Pharmacists should encourage patients to adopt lifestyle measures to reduce risk of GC-induced osteoporosis (see Box 3)7. Patients should be reminded not to stop treatments of oral GC suddenly, even if they are worried about their osteoporosis risk and should be encouraged to consult with their GP or specialist for further advice25–27.
Box 3: Lifestyle measures to reduce risk of GC-induced osteoporosis
- Encourage healthy, balanced diets that contain adequate calcium and vitamin D to promote bone resorption;
- Encourage smoking cessation and drinking alcohol according to NHS advice;
- Patients should be encouraged to stay physically active — within the limits of their underlying condition — to support bone health.
Where possible, localised GC should be used (i.e. inhalers, topical, enemas, joint injections), to mitigate risk of systemic absorption. Bisphosphonate medications (e.g. risedronate, alendronic acid) may be considered in patients with higher risk of fracture (e.g., individuals of increasing age, women, menopause, smoking, alcohol, previous fractures, parenteral history of hip fracture, body mass index of <18.5kg/m2)7,28.
What ‘sick day rules’ information do patients need?
Sick day rules provide information to patients on what to do if they have an acute illness or are due to undergo a surgical procedure. National Institute for Health and Care Excellence guidance, published in 2025, refers to information from the Society of Endocrinology; however, specific trust guidance should be checked first7,29. There are various situations in which an increase in GC is required owing to illness and the advice is based upon the patient’s current GC dose29. Patients may be advised to double their current dose or otherwise to split their dose to take half in the morning and half in the afternoon. Advice is also included for patients who are having planned surgery, where the clinical team must be informed beforehand of the patient’s GC use so that they can provide appropriate treatment throughout hospital admission.
As part of sick day rules guidance, it is essential to highlight to patients the importance of not stopping GC abruptly, other than in specific circumstances, such as with very short courses29. Patients should ensure they always have additional supply of GC in case they need to follow sick day guidance.
Patients at risk of adrenal insufficiency should receive a steroid emergency card (red), while blue steroid treatment cards are given only in specific circumstances (see Figure 230,31).
For more with details concerning steroid emergency and steroid treatment cards, see Figure 37.
Figure 2: Steroid emergency and steroid treatment cards
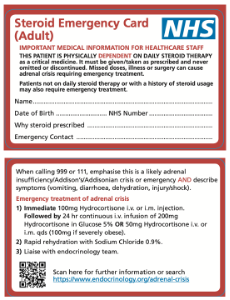
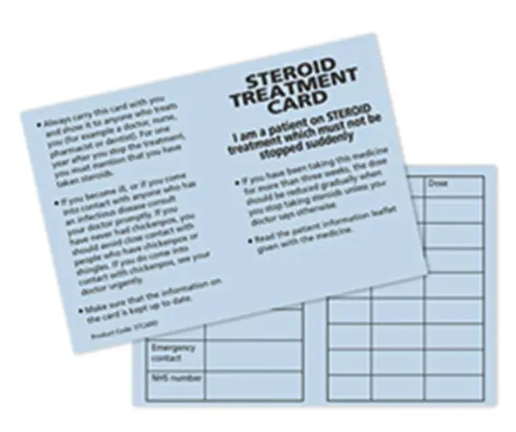
Figure 3: Summary of when patients require steroid emergency, sick day rules and/or treatment cards
Considerations for stopping and tapering steroids
Tapering oral GC should be individualised to the patient, with the rate and extent of dose reduction guided by clinical context. Important considerations include the underlying condition being treated, the duration of therapy and patient-specific factors, such as the risk of relapse and reported side effects.
Gradual withdrawal of systemic GC should be considered in the majority of patients whose disease is unlikely to relapse, which includes:
- Adults who have received more than 40mg prednisolone — or equivalent — daily for more than one week;
- Children and paediatrics who have received more than 40mg prednisolone daily for more than one week or 2mg/kg daily for one week or 1mg/kg daily for one month32,33.
Gradual withdrawal of GC should also be considered in the following patient scenarios:
- If the patient has been given repeat doses in the evening;
- If the patient received more than three weeks’ treatment;
- If the patient recently received repeated courses (particularly if taken for longer than three weeks);
- If the patient has taken a short course within one year of stopping long-term therapy;
- Other possible causes of adrenal suppression32,33.
In patients whose condition is unlikely to relapse and who have received treatment for three weeks or less and who are not included in the patient groups above, systemic GC may be stopped abruptly.
During GC withdrawal, the dose may be reduced rapidly down to physiological doses, which is equivalent to prednisolone 7.5mg daily in adults or prednisolone 2.0–2.5mg/m2 daily in children, and then reduced more slowly. Ongoing clinical assessment during tapering is essential to monitor for potential disease recurrence.
Best practice for any patient starting high-dose or long-term oral glucocorticoids
- Counsel patients on common side effects (e.g. infection, hypoglycaemia, gastrointestinal symptoms) and what to do if these occur;
- Ensure supportive medication (e.g. proton pump inhibitors) are provided as appropriate;
- Supply information regarding sick day rules as appropriate;
- Provide appropriate steroid emergency card and/ or steroid treatment card if required.
Useful resources
- British Society for Paediatric Endocrinology & Diabetes;
- ‘Steriod sick day rules’; Society for Endocrinology
- ‘Exogenous steroids treatment in adults‘ — combined guidance from Society for Endocrinology, British Association of Dermatologists, Specialist Pharmacy Service and the NHS.
- 1.Nicolaides NC, Kyratzi E, Lamprokostopoulou A, Chrousos GP, Charmandari E. Stress, the Stress System and the Role of Glucocorticoids. Neuroimmunomodulation. 2014;22(1-2):6-19. doi:10.1159/000362736
- 2.Barnes PJ. Anti-inflammatory Actions of Glucocorticoids: Molecular Mechanisms. Clinical Science. 1998;94(6):557-572. doi:10.1042/cs0940557
- 3.Hench PS, Kendall EC, Slocumb CH, Polley HF. Adrenocortical Hormone in Arthritis. Annals of the Rheumatic Diseases. 1949;8(2):97-104. doi:10.1136/ard.8.2.97
- 4.British National Formulary. Glucocorticoid and mineralocorticoid activity. National Institute for Health and Care Excellence . 2025. https://bnf.nice.org.uk/treatment-summaries/glucocorticoid-therapy/
- 5.Menzies-Gow A, Tran T, Stanley B, et al. Trends in Systemic Glucocorticoid Utilization in the United Kingdom from 1990 to 2019: A Population-Based, Serial Cross-Sectional Analysis. POR. 2024;Volume 15:53-64. doi:10.2147/por.s442959
- 6.Alam MM, Tariq M, Bondugulapati LNR, et al. Assessing the Knowledge of Sick-Day Rules Among Patients on Long-Term Glucocorticoids and Healthcare Professionals in a UK District General Hospital. Ibnosina Journal of Medicine and Biomedical Sciences. 2022;15(01):033-036. doi:10.1055/s-0042-1750181
- 7.Clinical Knowledge Summary (CKS) Scenario: Corticosteroids. National Institute for Health and Care Excellence. 2025. https://cks.nice.org.uk/topics/corticosteroids-oral/management/corticosteroids
- 8.Munson JC, Wahl PM, Daniel G, Kimmel SE, Hennessy S. Factors associated with the initiation of proton pump inhibitors in corticosteroid users. Pharmacoepidemiology and Drug. 2012;21(4):366-374. doi:10.1002/pds.2350
- 9.Hossam Abdelmonem B, Abdelaal NM, Anwer EKE, et al. Decoding the Role of CYP450 Enzymes in Metabolism and Disease: A Comprehensive Review. Biomedicines. 2024;12(7):1467. doi:10.3390/biomedicines12071467
- 10.Preissner S, Kroll K, Dunkel M, et al. SuperCYP: a comprehensive database on Cytochrome P450 enzymes including a tool for analysis of CYP-drug interactions. Nucleic Acids Research. 2009;38(suppl_1):D237-D243. doi:10.1093/nar/gkp970
- 11.Prednisolone interactions. National Institute for Health and Care Excellence. 2025. https://www.medicinescomplete.com/#/content/bnf/_656697437_interactions
- 12.George M, Joseph L, Sujith K, Georson G, Johnny O, Ku S. Effect of Corticosteroids on Serum Potassium Levels in Patients with Obstructive Airway Disorder. IJHSR. 2017. https://www.ijhsr.org/IJHSR_Vol.7_Issue.4_April2017/62.pdf
- 13.Gabriel SE, Jaakkimainen L, Bombardier C. Risk for Serious Gastrointestinal Complications Related to Use of Nonsteroidal Anti-inflammatory Drugs. Ann Intern Med. 1991;115(10):787-796. doi:10.7326/0003-4819-115-10-787
- 14.Prednesol 5mg Tablets. Advanz Pharma. 2024. https://www.medicines.org.uk/emc/product/14675/smpc
- 15.Steroids . NHS. 2025. https://www.nhs.uk/medicines/steroids/
- 16.British National Formulary for Children (BNF-C). Corticosteroids, general use. National Institute for Health and Care Excellence. 2025. https://bnfc.nice.org.uk/treatment-summaries/corticosteroids-general-use/
- 17.Prednisolone 5mg Tablets. Wockhardt UK Ltd. 2021. https://www.medicines.org.uk/emc/product/2427/smpc
- 18.Oral treatment with corticosteroids. British Association of Dermatologists. 2024. https://www.bad.org.uk/pils/oral-treatment-with-corticosteroids
- 19.Corticosteroids: rare risk of central serous chorioretinopathy with local as well as systemic administration. Medicines and Healthcare products Regulatory Agency. 2017. https://www.gov.uk/drug-safety-update/corticosteroids-rare-risk-of-central-serous-chorioretinopathy-with-local-as-well-as-systemic-administration
- 20.National Patient Safety Alert – Steroid Emergency Card to support early recognition and treatment of adrenal crisis in adults. NHS England . 2024. https://www.england.nhs.uk/publication/national-patient-safety-alert-steroid-emergency-card-to-support-early-recognition-and-treatment-of-adrenal-crisis-in-adults/
- 21.Adrenal Insufficiency Card. British Society for Paediatric Endocrinology and Diabetes. 2023. https://www.bsped.org.uk/media/jy4hfnni/bsped-ai-card-april-2023-v1-6-fillable.pdf
- 22.Yellow Card. Medicines and Healthcare products Regulatory Agency. https://yellowcard.mhra.gov.uk/
- 23.Contraindications and special considerations. UK Government . 2017. https://assets.publishing.service.gov.uk/media/5a82ce28e5274a2e8ab5970f/Greenbook_chapter_6.pdf
- 24.Nowotny H, Ahmed SF, et al. Therapy options for adrenal insufficiency and recommendations for the management of adrenal crisis. Endocrine. 2021;71(3):586-594. doi:10.1007/s12020-021-02649-6
- 25.Rosen H, Saag K. Prevention and treatment of glucocorticoid-induced osteoporosis. UpToDate. 2025. https://www.uptodate.com/contents/prevention-and-treatment-of-glucocorticoid-induced-osteoporosis
- 26.Kobza AO, Herman D, Papaioannou A, Lau AN, Adachi JD. Understanding and Managing Corticosteroid-Induced Osteoporosis. OARRR. 2021;Volume 13:177-190. doi:10.2147/oarrr.s282606
- 27.Steroids (Glucocorticoids) and Bone Health. Royal Osteoporosis Society. 2022. https://theros.org.uk/information-and-support/osteoporosis/causes/steroids/
- 28.Clinical Knowledge Summary (CKS) Osteoporosis – prevention of fragility fractures. National Institute for Health and Care Excellence. 2025. https://cks.nice.org.uk/topics/osteoporosis-prevention-of-fragility-fractures/
- 29.Steroid Sick Day Rules. Society for Endocrinology. https://www.endocrinology.org/media/4142/ai-and-exogenous-steroids_pis_final.pdf
- 30.Steroid Emergency Card (Adult). Society for Endocrinology. https://www.endocrinology.org/media/3873/steroid-card.pdf
- 31.Mitchell A, Walker L. Bringing Steroid Safety to the Masses. Endocrinologist. 2021. https://www.endocrinology.org/endocrinologist/142-winter-2021/features/bringing-steroid-safety-to-the-masses/
- 32.British National Formulary for Children (BNF-C): Prednisolone. National Institute for Health and Care Excellence. 2025. https://bnfc.nice.org.uk/drugs/prednisolone/
- 33.British National Formulary: Prednisolone. National Institute for Health and Care Excellence. 2025. https://bnf.nice.org.uk/drugs/prednisolone/


