VOISIN/PHANIE/SCIENCE PHOTO LIBRARY
After reading this learning article, you should be able to:
- Identify the causes of carpal tunnel syndrome;
- Describe the symptoms of carpal tunnel syndrome;
- Outline the treatment options available;
- Apply knowledge of carpal tunnel syndrome to the community pharmacy setting;
- Understand when referral to another healthcare professional may be required.
Carpal tunnel syndrome (CTS) is caused by compression of the median nerve at the wrist as it passes through the carpal tunnel, an anatomical passageway connecting the wrist and forearm[1]. CTS can present as sensory and motor symptoms or pain in the thumb and fingers[2].
CTS most commonly affects people aged over 45 years, with a peak incidence at 46–60 years, and has a higher prevalence among women[3,4]. Risk factors include pregnancy; occupations such as construction, mining and computer-based roles; and history of wrist injury through repetitive strain, soft-tissue trauma or fracture[5,6]. Described as an “occupational overuse syndrome” or a “technological disease”, the incidence of CTS is rising in the UK, with its prevalence in the UK between 7–16%. CTS accounts for 90% of all peripheral neuropathies and its lifetime risk increases from 10% to 84% in patients with type 1 diabetes mellitus[4,7,8].
CTS often develops insidiously, becoming a chronic condition that severely impinges on patients’ ability to carry out daily activities. The pain associated with the condition has a detrimental impact on quality of life[9]. Late diagnosis of CTS is linked to poorer long-term outcomes, even after surgical intervention; therefore, prompt recognition with minimal delays to management is imperative[10].
While severe cases will ultimately require specialist management, mild-to-moderate cases can be effectively managed in primary care[11]. The accessibility of pharmacies, coupled with the number of patients seeking over-the-counter remedies for undiagnosed hand or wrist pain, means that pharmacists must be able to confidently identify CTS and recommend appropriate treatment and/or referral.
The role of the pharmacist includes providing advice on self-management of the condition, the provision of wrist splints and supporting patients with mild symptoms — advising them to return if the disease progresses. In more severe cases, patients can be referred to their GP for management or onward referral, where indicated. Pharmacists can help patients with CTS access treatment, manage their symptoms and delay the need for surgical intervention[12].
This article outlines the clinical presentation, diagnosis and treatment of CTS, with a focus on identification and management within a community pharmacy setting.
Anatomy
The anatomy of the hand is complex, permitting a greater degree of manual dexterity compared with other animals[13]. Many of the hand muscles originate within the forearm to generate full range of movement[14].
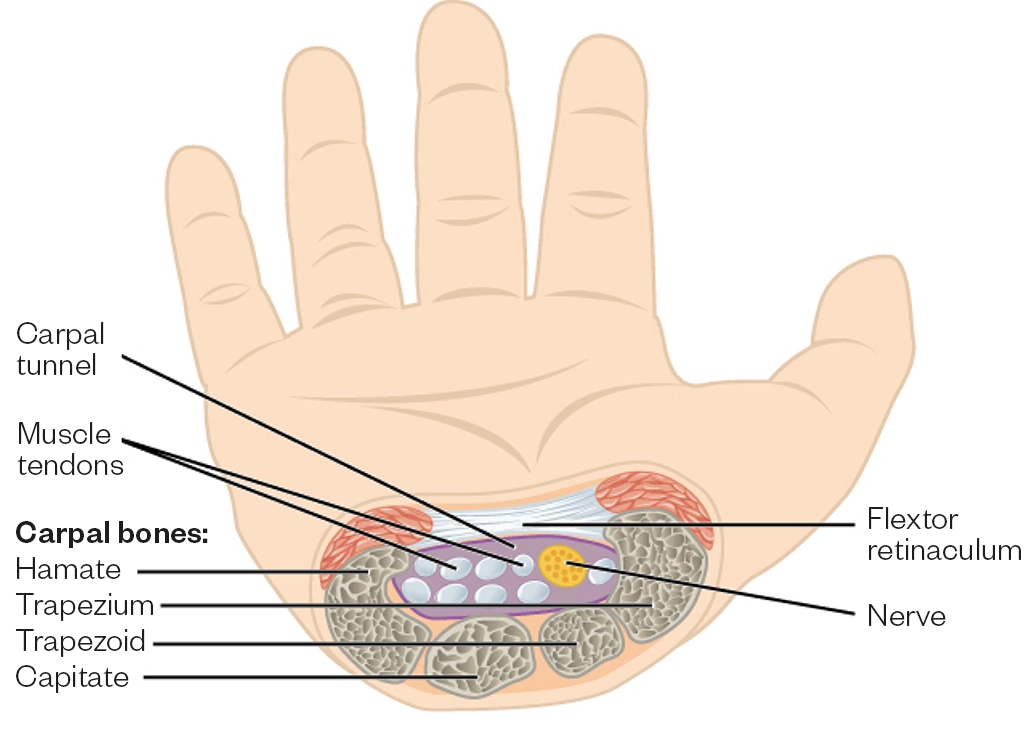
The borders of the carpal tunnel, which runs between the forearm and hand, consist of the carpal, or wrist bones, and the flexor retinaculum — a sheet of connective tissue that lies just underneath the skin of the wrist, below the palm (see Figure 1). Together, these boundaries produce a narrow tunnel through which several structures — crucial for manipulation of the hand — pass through[15]. These structures include the median nerve and the tendons of the flexor muscles within the forearm, which allow for flexion of the thumb and fingers — important for grasping and pinching. The median nerve provides sensory innervation to the palmar, thumb, index and middle fingers, as well as the lateral half of the ring finger, and motor innervation to several key muscles of the hand (lateral lumbrical muscles) and thumb (opponens pollicis, abductor pollicis and flexor pollicis brevis)[14].
Aetiology and risk factors
The size of structures passing through the carpal tunnel play an important part in predisposition for CTS[17]. Factors contributing to the development of CTS can be divided into those affecting the container (i.e. the carpal tunnel itself) or those affecting the contents of the carpal tunnel[18].
Factors affecting the container include instances where the diameter of the carpal tunnel is too small (anthropometric factors). On a population level, there is natural variation in the size of the carpal tunnel. Female gender is associated with a smaller carpal arch and increased risk of CTS[4]. Fractures of the carpal bones or radial head and inflammation owing to arthritis may also affect the diameter of the carpal tunnel[6].
Factors affecting the contents of the carpal tunnel include pathologies where the structures within the tunnel are increased in size, such as flexor tendon hypertrophy. This can occur because of exposure to vibrating tools or machinery (e.g. the mining and road repair industries). Tendon hypertrophy can also occur secondary to repetitive hand movements and computer work, or previous injury, such as a wrist fracture[5]. Pregnancy, renal failure and hypothyroidism can also cause a change to the contents of the carpal tunnel by causing a shift in fluid distribution[19,20]. Type 2 diabetes mellitus and gout can cause metabolic tenosynovitis, resulting in inflammation to the flexor tendons of the forearm[21,22].
Genetics is the single strongest risk factor in women[5,23]. In both genders, body mass index (BMI) is a risk factor, affecting both the container and the contents of the carpal tunnel[22]. Greater levels of adipose tissue within the wrist will exert a greater pressure on the carpal tunnel, and obesity is linked with greater levels of pro-inflammatory cytokines, which may increase the risk of flexor tendon hypertrophy[24].
Pathophysiology
Compression of the median nerve within the carpal tunnel creates an entrapment neuropathy, causing chronic insult to the nerve over time. The increased pressure around the nerve affects the microcirculation, resulting in ischaemic damage, demyelination and axon degeneration[25]. Nerve conduction slows and, as ion channels undergo pathological changes, ectopic action potentials can occur leading to paraesthesia, sensory changes and shock-like pains. This damage can result in a localised lesion on the nerve[25].
In severe cases, the blood supply and drainage of the hand can also be affected. Inflammation and redness, caused by increased pressure in the carpal tunnel, reduced venous outflow and local oedema, can worsen the nerve entrapment and lead to a further decrease in function[25].
Signs and symptoms
CTS is a varied disease that affects each patient individually. While no single symptom is recognised as being diagnostic, some are reported more frequently than others and may affect one or both hands at presentation[26]. The most common symptoms are neuropathic pain in the wrist and hand, described as ‘shock-like waves’, which may also travel from the wrist to the top of the arm, as far as the shoulder. Patients may also report difficulty with fine motor movement and gripping objects.
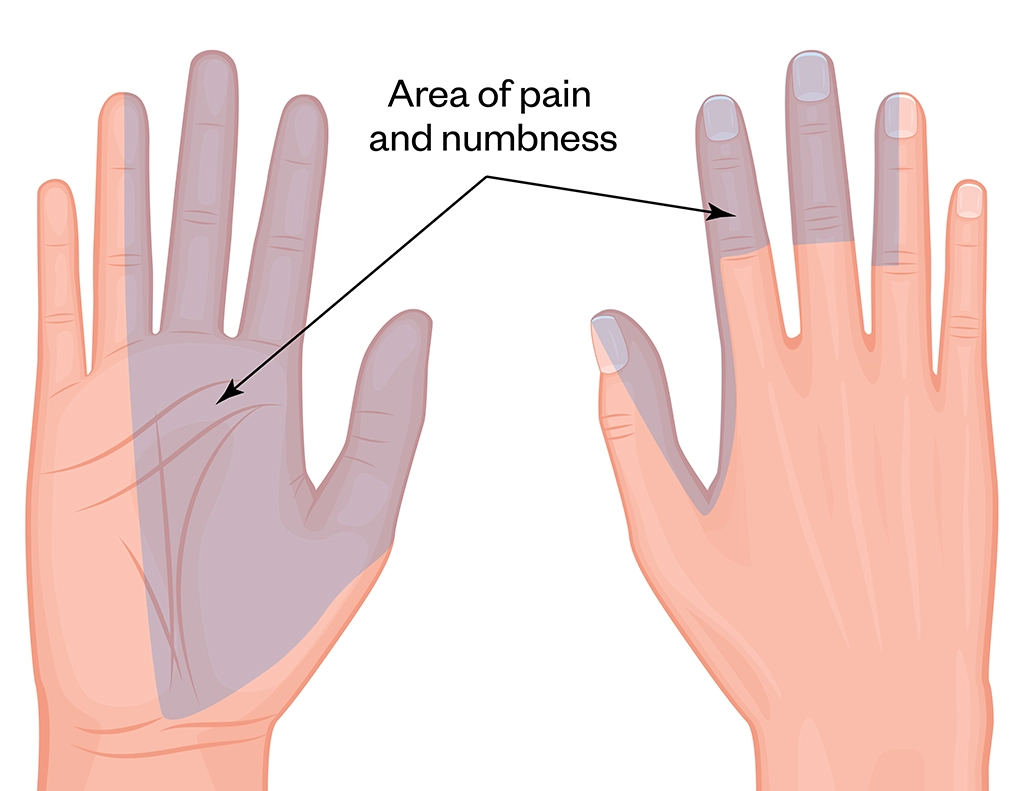
Patients may report tingling and numbness in the thumb, index and middle fingers in the distribution of the median nerve, and/or a tightness, hotness or dryness of their hand(s)[1,27]. Symptoms are often worse at night, causing sleep disruption, but may become more continuous, as CTS persists if left untreated[25]. Patients may complain of worsening symptoms with repetitive hand movements, or sustained hand or wrist positions. Change of hand position or shaking the wrist is reported to alleviate symptoms. Patients may demonstrate the ‘flick sign’ — where they can be observed to shake one or both hands as if to flick water from them — a clinical sign which is 93% sensitive and 96% specific for CTS[28].
Pharmacists should be aware of the following red flag symptoms, and ensure the patient is referred for urgent assessment:
- Facial drooping, slurred speech and unilateral arm weakness that is indicative of stroke;
- Chest pain, breathlessness, pain radiating to jaw, arm or shoulder that is indicative of myocardial infarction;
- Weakness in other limbs, slurred speech, weight loss, reduced grip, muscle twitches that is indicative of motor neurone disease;
- Fatigue, blurred vision, urinary frequency, muscle spasms, reduced cognition, reduced ability to walk that is indicative of multiple sclerosis.
Shutterstock.com
CTS may result in weakness of the muscles of the hand, with resultant muscular atrophy — symptoms of which may include loss of grip strength and dexterity, with frequent dropping of items; difficulty with fine motor tasks, such as fastening shirt buttons; and a loss of proprioception. In advanced cases of CTS, impingement of the median nerve reduces the motor innervation of the nerve to the muscles of the thenar eminence (muscles at the base of the thumb). This can lead to thenar eminence wasting, as these muscles are unable to move, and is characterised by an indent over the thumb base (see Figure 3)[29]. There may also be dryness of skin on examination, a secondary consequence of reduced finger sweating owing to a reduction in sympathetic tone in the region of the hand innervated by the median nerve[30].

MIKE DEVLIN/SCIENCE PHOTO LIBRARY
Diagnosis and investigations
CTS is a largely clinical diagnosis, based on the presence of the typical symptoms and clinical signs, in combination with a thorough history (see Box). There are several additional tests that can be used to aid in the diagnosis of CTS, all of which can be performed in a community pharmacy setting[27]. Each of these tests involves the clinician performing a simple manoeuvre designed to exacerbate symptoms of the underlying CTS, which should be interpreted in the context of the clinical history and prior examination[11,31,32]. Any pain or paraesthesia experienced by the patient during the following tests may be indicative of CTS.
Box: Suggested questions for investigating a suspected case of carpal tunnel syndrome
History and examination
- Do you ever get numbness or tingling in one or both hands below the wrist?
- Does this sensation mostly affect part of the thumb, the index and middle finger, and part of the ring finger?
- How long have you had these symptoms for?
- Are there any activities which make the symptoms better or worse?
- Is the sensation in your hands relieved by flicking them at the wrist?
- Are the symptoms better or worse at any time of day?
- Do they affect one side of the body, or both?
- Do you find you drop things more than you used to?
- Do you find tasks requiring fine movement (such as fastening buttons) difficult?
- What do you do for a living?
- Have you noticed any change or reduction in the size of the muscle at the base of your thumb?
A positive response to all questions would indicate a very stereotypical presentation of CTS. Negative responses to one or more of the above questions do not rule out a CTS diagnosis and should be considered in the broader context of history and investigations as outlined below.
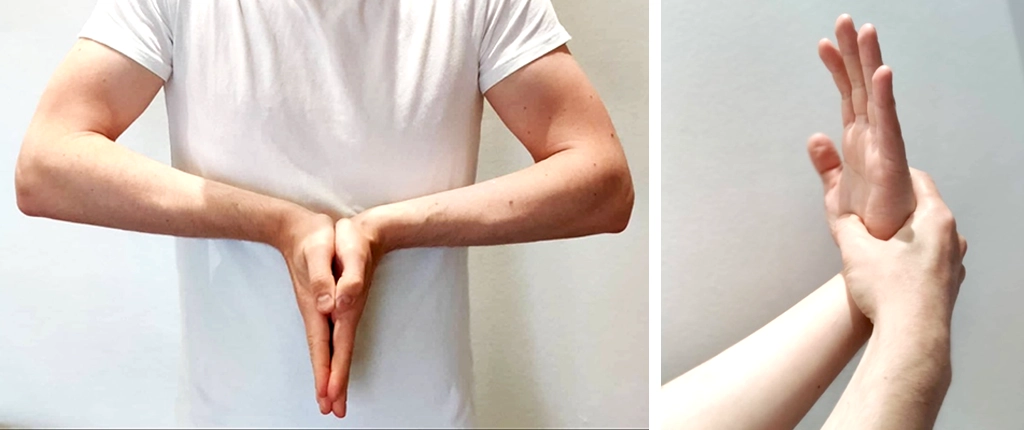
Phalen’s test
Flexing the wrist for 60 seconds produces pain or paraesthesia in the median nerve distribution in CTS. This test is typically performed either with the patient flexing their own wrists by placing the backs of the hands together or by the clinician passively flexing the patient’s wrist (see Figure 4)[33].
Images courtesy of Paterson and Pinedo
Tinel’s test
Tapping repeatedly over the median nerve at the wrist produces pain or paraesthesia in the median nerve distribution in CTS[33].
Images courtesy of Paterson and Pinedo
Durkan’s test (carpal tunnel compression test)
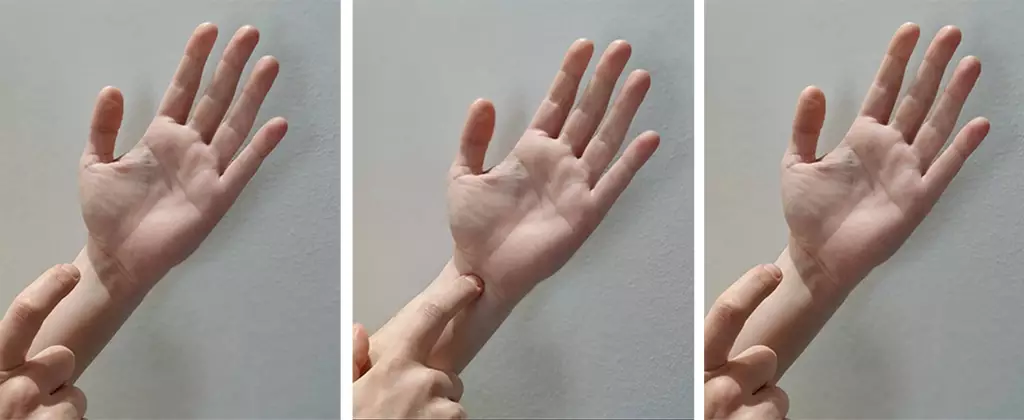
Also known as the carpal tunnel compression test, pressure is applied over the proximal edge of the carpal ligament (the proximal wrist crease), which produces or worsens paraesthesia in the median nerve distribution in CTS[34].

Images produced courtesy of Paterson and Pinedo
Differential diagnoses that may present in a similar way to CTS include: osteoarthritis and inflammatory arthritides; Raynaud’s disease; cervical radiculopathy; neuropathy secondary to diabetes mellitus; hypothyroidism and B12 deficiency; contact dermatitis; multiple sclerosis; and stroke[35,36]. If a specific underlying cause for CTS is suspected (such as type 2 diabetes mellitus or hypothyroidism), further investigation by means of the relevant blood tests is indicated[11].
Management and referral
Many of the recommended interventions for patients with CTS can be provided in primary care. Pharmacists should refer all suspected cases to a GP for formal diagnosis. More severe cases may then warrant onward referral to specialist care for further investigation (e.g. if the symptoms are severe or functional ability is reduced; if symptoms recur following carpal tunnel surgery; if conservative management fails; or if underlying neurological disease, inflammatory joint disease, peripheral limb ischaemia, or cervical nerve root entrapment is suspected)[11]. Further investigations may include imaging (such as ultrasound or MRI) or electrophysiological studies, including nerve conduction studies and electromyograms (EMG)[11]. Nerve conduction studies measure neuronal impulses to determine how well the median nerve is conducting. An EMG focuses on the muscle target groups and detects electrical activity in those muscles, determining if the nerve is effectively conducting a signal[37].
Conservative management
Early management using conservative approaches is crucial, regardless of severity of disease, and is linked with improved outcomes, such as reduced recurrence of symptoms and delayed need for surgical intervention.
Pharmacists should counsel patients on lifestyle modification, such as avoiding repetitive manual movements or tasks which precipitate symptoms. If an occupational cause is suspected, the patient should be advised to seek an assessment with their employer to alter their work environment or duties (e.g. keyboard rests fitted, reduced exposure to vibrating machinery if at risk)[11,38]. Pharmacists should also consider referral to a physiotherapist or recommend that patients self-refer, depending on local service provision and referral pathways.
Wrist splints can be sold over the counter and help maintain carpal tunnel stability. They are particularly useful overnight if patients report symptoms triggered by their sleeping positions[11].
Pharmacological strategies
Non-steroidal anti-inflammatory drugs are not indicated in carpal tunnel syndrome as they are no more effective than placebo[39].
Application of EMLA cream (Aspen; lidocaine 2.5%, prilocaine 2.5%) can provide patients with some symptomatic relief while they wait for an appointment with their GP or specialist; however, in rare cases, continuous use has been linked to methaemoglobinemia, therefore it should be used sparingly[40]. Care should be taken to ensure the patient does not have an allergy to either lidocaine or prilocaine. EMLA cream is a pharmacy medicine and can be purchased under the supervision of a pharmacist, although it is not licensed for symptomatic relief of CTS[41].
Corticosteroids, such as methylprednisolone (4–80mg) injected locally into the carpal tunnel, just beneath the flexor retinaculum, can provide benefit for 10–12 weeks post-injection[42]. This procedure may be carried out in primary care, if service provision permits, or by a specialist once referred[43]. Injected steroids are preferred over oral steroids for the same indication, as they have a much longer duration of action and a more localised effect[43].
Surgical intervention
In severe cases where conservative measures have been unsuccessful, or pain persists and/or muscle weakness is present, surgical intervention may be required to provide relief and prevent further disease progression[11]. A carpal tunnel release can be performed as a day-case procedure, using local or regional anaesthesia. Surgical intervention has been shown to be highly efficacious, with around one third of patients reporting a complete elimination of symptoms, and a further third reporting a major improvement in symptoms[38].
Follow up
It is advisable for patients with moderate-to-severe symptoms to return to their GP for follow up, as it is a more appropriate setting for further management. Patients with mild symptoms may return to the pharmacy if symptoms worsen, or may return to the pharmacy when collecting their next prescription, providing the opportunity for further discussion of their symptoms.
- 1Katz JN, Simmons BP. Carpal Tunnel Syndrome. N Engl J Med 2002;346:1807–12. doi:10.1056/nejmcp013018
- 2Nora DB, Becker J, Ehlers JA, et al. Clinical features of 1039 patients with neurophysiological diagnosis of carpal tunnel syndrome. Clinical Neurology and Neurosurgery 2004;107:64–9. doi:10.1016/j.clineuro.2004.08.003
- 3Sevy J, Varacallo M. Carpal Tunnel Syndrome. StatPearls. 2021.http://www.ncbi.nlm.nih.gov/books/NBK448179/ (accessed Oct 2021).
- 4Bongers F, Schellevis F, van den, et al. Carpal tunnel syndrome in general practice (1987 and 2001): incidence and the role of occupational and non-occupational factors. Br J Gen Pract 2007;57:36–9.https://www.ncbi.nlm.nih.gov/pubmed/17244422
- 5Ali KM, Sathiyasekaran BWC. Computer Professionals and Carpal Tunnel Syndrome (CTS). International Journal of Occupational Safety and Ergonomics 2006;12:319–25. doi:10.1080/10803548.2006.11076691
- 6Yeh K-T, Lee R-P, Yu T-C, et al. Risk factors for carpal tunnel syndrome or trigger finger following distal radius fracture: a nationwide study. Sci Rep 2020;10. doi:10.1038/s41598-020-57415-x
- 7TiricCampara M, Krupic F, Biscevic M, et al. Technological Diseases: Carpal Tunnel Syndrome, a Mouse Shoulder, Cervical Pain Syndrome. Acta Inform Med 2014;22:333. doi:10.5455/aim.2014.22.333-340
- 8Singh R, Gamble G, Cundy T. Lifetime risk of symptomatic carpal tunnel syndrome in Type 1 diabetes. Diabet Med 2005;22:625–30. doi:10.1111/j.1464-5491.2005.01487.x
- 9Damms NA, McCallum LM, Sarrigiannis PG, et al. Pain as a determinant of health-related quality of life in patients with carpal tunnel syndrome; a case-controlled study. Postgraduate Medicine 2019;132:52–5. doi:10.1080/00325481.2019.1694840
- 10Masud M, Rashid M, Malik S, et al. Does the Duration and Severity of Symptoms Have an Impact on Relief of Symptoms after Carpal Tunnel Release? J Brachial Plex Peripher Nerve Inj 2019;14:e1–8. doi:10.1055/s-0038-1668552
- 11Carpal tunnel syndrome. National Institute for Health and Care Excellence. 2021.https://cks.nice.org.uk/topics/carpal-tunnel-syndrome/ (accessed Oct 2021).
- 12Phillips MR, Chang Y, Zura RD, et al. Impact of COVID-19 on orthopaedic care: a call for nonoperative management. Therapeutic Advances in Musculoskeletal 2020;12:1759720X2093427. doi:10.1177/1759720×20934276
- 13MARZKE MW, MARZKE RF. Evolution of the human hand: approaches to acquiring, analysing and interpreting the anatomical evidence. J Anatomy 2000;197:121–40. doi:10.1046/j.1469-7580.2000.19710121.x
- 14Moore K, Dalley A. Clinically Oriented Anatomy. India: : Wolters Kluwer 2018.
- 15LOWE BD. Effect of carpal tunnel syndrome on grip force coordination on hand tools. Ergonomics 1999;42:550–64. doi:10.1080/001401399185469
- 16Betts J, Desaix P, Johnson E, et al. Anatomy & Physiology. Texas: : Rice University 2013.
- 17Armstrong T, Castelli W, Evans F, et al. Some histological changes in carpal tunnel contents and their biomechanical implications. J Occup Med 1984;26:197–201.https://www.ncbi.nlm.nih.gov/pubmed/6716187
- 18Aboonq M. Pathophysiology of carpal tunnel syndrome. Neurosciences (Riyadh) 2015;20:4–9.https://www.ncbi.nlm.nih.gov/pubmed/25630774
- 19Finsen V, Zeitlmann H. Carpal tunnel syndrome during pregnancy. Scandinavian Journal of Plastic and Reconstructive Surgery and Hand Surgery 2006;40:41–5. doi:10.1080/02844310500410351
- 20Solomon DH, Katz JN, Bohn R, et al. Nonoccupational risk factors for carpal tunnel syndrome. J Gen Intern Med 1999;14:310–4. doi:10.1046/j.1525-1497.1999.00340.x
- 21Rich JT, Bush DC, Lincoski CJ, et al. Carpal Tunnel Syndrome Due To Tophaceous Gout. Orthopedics 2004;27:862–3. doi:10.3928/0147-7447-20040801-23
- 22Becker J, Nora DB, Gomes I, et al. An evaluation of gender, obesity, age and diabetes mellitus as risk factors for carpal tunnel syndrome. Clinical Neurophysiology 2002;113:1429–34. doi:10.1016/s1388-2457(02)00201-8
- 23Hakim AJ, Cherkas L, El Zayat S, et al. The genetic contribution to carpal tunnel syndrome in women: A twin study. Arthritis & Rheumatism 2002;47:275–9. doi:10.1002/art.10395
- 24Tomlinson DJ, Erskine RM, Morse CI, et al. The combined effects of obesity and ageing on skeletal muscle function and tendon properties in vivo in men. Endocrine 2021;72:411–22. doi:10.1007/s12020-020-02601-0
- 25Bland JD. Carpal tunnel syndrome. Current Opinion in Neurology 2005;18:581–5. doi:10.1097/01.wco.0000173142.58068.5a
- 26Padua L, Lo Monaco M, Padua R, et al. Neurophysiological classification of carpal tunnel syndrome: assessment of 600 symptomatic hands. Ital J Neuro Sci 1997;18:145–50. doi:10.1007/bf02048482
- 27Katz JN. The Carpal Tunnel Syndrome: Diagnostic Utility of the History and Physical Examination Findings. Ann Intern Med 1990;112:321. doi:10.7326/0003-4819-112-5-321
- 28Wipperman J, Goerl K. Carpal Tunnel Syndrome: Diagnosis and Management. Am Fam Physician 2016;94:993–9.https://www.ncbi.nlm.nih.gov/pubmed/28075090
- 29Claes F, Kasius KM, Meulstee J, et al. Comparing a New Ultrasound Approach with Electrodiagnostic Studies to Confirm Clinically Defined Carpal Tunnel Syndrome. American Journal of Physical Medicine & Rehabilitation 2013;92:1005–11. doi:10.1097/phm.0b013e31829b4bd8
- 30Kuwabara S, Tamura N, Yamanaka Y, et al. Sympathetic sweat responses and skin vasomotor reflexes in carpal tunnel syndrome. Clinical Neurology and Neurosurgery 2008;110:691–5. doi:10.1016/j.clineuro.2008.04.004
- 31Naranjo A, Ojeda S, Mendoza D, et al. What is the diagnostic value of ultrasonography compared to physical evaluation in patients with idiopathic carpal tunnel syndrome? Clin Exp Rheumatol 2007;25:853–9.https://www.ncbi.nlm.nih.gov/pubmed/18173919
- 32Priganc VW, Henry SM. The Relationship among Five Common Carpal Tunnel Syndrome Tests and the Severity of Carpal Tunnel Syndrome. Journal of Hand Therapy 2003;16:225–36. doi:10.1016/s0894-1130(03)00038-3
- 33Kuschner S, Ebramzadeh E, Johnson D, et al. Tinel’s sign and Phalen’s test in carpal tunnel syndrome. Orthopedics 1992;15:1297–302.https://www.ncbi.nlm.nih.gov/pubmed/1461811
- 34Durkan J. A new diagnostic test for carpal tunnel syndrome. J Bone Joint Surg Am 1991;73:535–8.https://www.ncbi.nlm.nih.gov/pubmed/1796937
- 35LeBlanc K, Cestia W. Carpal tunnel syndrome. Am Fam Physician 2011;83:952–8.https://www.ncbi.nlm.nih.gov/pubmed/21524035
- 36Middleton SD, Anakwe RE. Carpal tunnel syndrome. BMJ 2014;349:g6437–g6437. doi:10.1136/bmj.g6437
- 37Lo JK, Finestone HM, Gilbert K, et al. Community-based referrals for electrodiagnostic studies in patients with possible carpal tunnel syndrome: What is the diagnosis? Archives of Physical Medicine and Rehabilitation 2002;83:598–603. doi:10.1053/apmr.2002.32476
- 38Multanen J, Uimonen MM, Repo JP, et al. Use of conservative therapy before and after surgery for carpal tunnel syndrome. BMC Musculoskelet Disord 2021;22. doi:10.1186/s12891-021-04378-3
- 39Gerritsen AAM, de Krom MCTFM, Struijs MA, et al. Conservative treatment options for carpal tunnel syndrome: a systematic review of randomised controlled trials. Journal of Neurology 2002;249:272–80. doi:10.1007/s004150200004
- 40Hahn I-H, Hoffman RS, Nelson LS. EMLA®-induced methemoglobinemia and systemic topical anesthetic toxicity. The Journal of Emergency Medicine 2004;26:85–8. doi:10.1016/j.jemermed.2003.03.003
- 41Moghtaderi A, Jazayeri S, Azizi S. EMLA cream for carpal tunnel syndrome: how it compares with steroid injection. Electromyogr Clin Neurophysiol 2009;49:287–9.https://www.ncbi.nlm.nih.gov/pubmed/19845100
- 42Atroshi I, Flondell M, Hofer M, et al. Methylprednisolone Injections for the Carpal Tunnel Syndrome. Ann Intern Med 2013;159:309. doi:10.7326/0003-4819-159-5-201309030-00004
- 43Marshall SC, Tardif G, Ashworth NL. Local corticosteroid injection for carpal tunnel syndrome. Cochrane Database of Systematic Reviews Published Online First: 18 April 2007. doi:10.1002/14651858.cd001554.pub2