

This content was published in 2011. We do not recommend that you take any clinical decisions based on this information without first ensuring you have checked the latest guidance.
Summary
Liver disease can be classed as acute if the onset of symptoms does not
exceed six months or chronic if symptoms persist beyond this period.
In the initial stages of liver disease, inflammatory (hepatitis) or fatty
(steatosis) changes, or both (steatohepatitis), can occur. If the cause of
liver injury is not removed, the damage can progress to fibrosis and
eventually cirrhosis.
Fatigue, reduced appetite and weight loss are common symptoms of liver disease. Clinical features of chronic liver disease include jaundice, coagulopathy, encephalopathy, portal hypertension, varices and ascites.
Liver disease is one of the most common causes of death in England. Its increasing incidence is largely driven by preventable lifestyle factors, such as drinking excessive amounts of alcohol, obesity and behaviours leading to infection with hepatitis B and C. Currently, liver disease costs the NHS £460m a year[1].
The liver
The liver is the largest internal organ in the body. It is located in the right upper quadrant of the abdominal cavity below the diaphragm and normally weighs around 1.4kg in women and 1.6kg in men.
The liver is divided into two main lobes — the right lobe is much larger than the left. These lobes are further subdivided into smaller lobules. Each lobule is made up of millions of cells called hepatocytes, which are the basic
metabolic cells of the liver.
The liver is highly vascular. Most of its blood supply (80%) comes from the hepatic portal vein, which delivers blood containing digested nutrients from the small intestine. The other 20% is supplied by the hepatic artery, which branches from the aorta and supplies the liver with oxygen. These large blood vessels further subdivide into capillaries to supply blood to each of the lobules.
Functions of the liver
The liver is one of the busiest organs in the body, with most of its functions carried out by hepatocytes.
Functions of the liver include:
- Metabolism of carbohydrates, protein, fat, thyroxine (to active triiodothyronine), bilirubin, insulin, medicines, hormones (eg, prednisone to prednisolone), aldosterone and vitamins;
- Synthesis of plasma proteins (eg, albumin), clotting factors (eg, fibrinogen), cholesterol, glucose, bile, amino acids and urea;
- Storage of fat soluble vitamins (A, D, E and K) and glycogen;
- Regulating blood sugar;
- Immunity (the liver contains over half of the body’s macrophages).
Liver disease
Liver disease is a broad term describing any disease that affects the liver and can be classified as acute or chronic.
Acute liver disease
If the onset of symptoms does not exceed six months then a patient is deemed to have acute liver disease. Most cases are self-limiting episodes of hepatocyte inflammation or damage, which resolve without causing further complications.
In some rare cases the damage is so severe that it affects the whole liver leading to acute liver failure. These cases are associated with a high mortality and may require liver transplantation.
Chronic liver disease
Patients with symptoms of liver disease that persist for more than six months have chronic liver disease. It occurs when permanent structural changes within the liver occur secondarily to longstanding hepatocyte damage.
Causes of liver disease
Alcohol
Alcohol consumption is a major risk factor for the development of liver disease. However, clear evidence about the relationship between the amount of alcohol a person drinks and the incidence of liver disease is lacking. For further information about the effects of alcohol on the liver, see the accompanying article (p149).
Viral infection
There are several viruses that can cause hepatitis.
Hepatitis A is spread via the faecal-oral route and is more prevalent in areas where hygiene standards and sanitation are poor. The infection does not progress to chronic liver disease or to carrier status (ie, once a person has recovered they can no longer pass on the virus).
Hepatitis B can cause acute illness or chronic infection and, despite the availability of a highly effective vaccine and improvements in antiviral therapy, it remains a major public health problem globally. Transmission occurs through contact with infected blood or body fluids and it is commonly passed from an infected mother to her child during birth.
When exposure to the virus occurs early in life the likelihood of chronic infection is high (90%) compared with less than 5–10% for adults who acquire the infection.
Hepatitis C is a blood-borne virus that is commonly transmitted through sharing equipment for injectable drug use. It was also spread through blood transfusion before the introduction of screening in 1991. There is a small risk of hepatitis C infection associated with tattooing, electrolysis, ear piercing, acupuncture and transmission from mother to baby.
After exposure to the hepatitis C virus patients are generally asymptomatic, although about 20% will develop acute hepatitis and may experience malaise, weakness and anorexia. About 85% of people exposed to the virus develop chronic disease. Around 20–30% of patients with chronic hepatitis C infection progress to end-stage liver disease within 20 years and a small proportion develop hepatocellular carcinoma.
Hepatitis D is also known as delta virus and can only replicate in the presence of the hepatitis B virus. The combination of both increases the risk of progression to chronic hepatitis and cirrhosis.
Hepatitis E is transmitted via the faecal-oral route. Unless a patient has pre-existing liver disease the infection is generally mild and lasts only a couple of weeks. Hepatitis E does not cause chronic infection.
Non-alcoholic fatty liver disease
In non-alcoholic fatty liver disease, triglycerides accumulate within hepatocytes (steatosis) in the absence of excessive alcohol consumption. This steatosis can cause hepatocyte inflammation, in which case it is termed non-alcoholic steatohepatitis.
Medicines
Many medicines have been implicated as causes of liver dysfunction (in therapeutic or toxic doses). This can be a consequence of either direct toxicity of the drug or toxicity of metabolites. Generally, patients with pre-existing liver disease are not at increased risk of drug induced hepatotoxicity (except from methotrexate and sodium valproate). Drugs can induce almost all forms of acute or chronic liver disease. In most cases withdrawal of the drug will lead to resolution of the liver damage.
Generally, patients with pre-existing liver disease are not at increased risk of drug induced hepatotoxicity
Genetic disorders
There are various inherited metabolic disorders that can affect the functioning of the liver, including:
- Haemochromatosis — the body absorbs an excessive amount of iron from the diet, which is then deposited in various organs, mainly the liver; iron stored in the liver can cause hepatocyte damage that may progress from hepatitis to liver cirrhosis;
- Wilson’s disease — copper accumulates in the body (mainly in the liver and brain), which can cause hepatitis, fibrosis and cirrhosis;
- Alpha-1 antitrypsin deficiency — leads to lung and liver disease; this is the most common genetic cause of liver dysfunction in children.
Immunological disorders
Abnormalities in immune function can also cause liver disease.
Autoimmune hepatitis can present as mild hepatitis, severe acute
hepatitis or as established cirrhosis. Typically, autoimmune hepatitis affects young women — the usual age of onset is between 20 and 40 years. Diagnosis is based on serum biochemistry, liver histology and the presence of certain antibodies (eg, antinuclear antibody).
Primary biliary cirrhosis is characterised by the progressive destruction of the small and intrahepatic bile ducts, which causes the accumulation of bile in the liver, damaging hepatocytes and leading to fibrosis and cirrhosis.
Primary sclerosing cholangitis is an uncommon chronic liver disease in which the intrahepatic or extrahepatic bile ducts progressively decrease in size due to inflammation and fibrosis. The disease is frequently associated with inflammatory diseases of the colon, especially ulcerative colitis.
Bile that is normally carried by these ducts accumulates within the liver and causes damage to the hepatocytes, hepatic inflammation and scarring. Over many years the scarring can affect the whole liver, causing
cirrhosis.
Malignancy
The most common primary malignant tumour of the liver is hepatocellular carcinoma, with most cases occurring secondary to viral hepatitis (B or C) or cirrhosis.
Structural abnormalities
Biliary atresia occurs where the bile ducts are damaged or blocked and results from a congenital malformation of the extrahepatic bile ducts. It causes progressive jaundice usually from the second week of life. If surgical intervention at this stage is unsuccessful then the condition is likely to progress to fibrosis and cirrhosis.
In children, biliary atresia is one of the most common causes of chronic liver disease and is the most common indication for liver transplantation.
Stages of liver disease
When the liver comes into contact with viruses or toxins, inflammatory (hepatitis) or fatty (steatosis) changes, or both (steatohepatitis), can occur. At this stage of liver disease the liver can still regenerate and these changes are usually reversible. If the cause of liver injury is not removed, the damage can progress to fibrosis and eventually cirrhosis of the liver.
Fibrosis
Liver fibrosis refers to the accumulation of tough, fibrous scar tissue in the liver. The necrosis of hepatocytes stimulates immune cells to release cytokines, growth factors and various unknown chemicals. These chemical messengers direct hepatic stellate cells (support cells in the liver) to activate and produce collagen, glycoproteins (such as fibronectin) and proteoglycans among other substances. These substances are deposited in the liver, causing the build-up of non-functional connective tissue, termed “extracellular matrix”.
At the same time, the process of breaking down or degrading collagen is impaired. In a healthy liver, the synthesis (fibrogenesis) and breakdown (fibrolysis) of matrix tissue are in balance. Fibrosis occurs when excessive scar tissue builds up faster than it can be broken down and removed from the liver.
Cirrhosis
Liver fibrosis can become so extensive that the architecture of the liveris altered — thisis called cirrhosis. As cirrhosis develops, scar tissue replaces healthy liver cells. The usual smooth texture of the liver becomes nodular causing the free flow of blood throughout it to be compromised, thus reducing the ability of the liver to perform its many functions.
Cirrhosis is divided into two categories:
- Compensated — this means that the liver is heavily scarred but is still able to cope with the damage and carry out most of its functions; a large proportion of people with compensated cirrhosis experience few or no symptoms;
- Decompensated — this means that the liver is extensively scarred and unable to function properly; patients with decompensated cirrhosis develop a range of symptoms and disease complications.
Clinical features
Fatigue, loss of appetite and weight loss are common symptoms of liver disease. Abdominal discomfort and tenderness can occur in patients with enlarged livers and, in chronic liver disease, swelling of the abdomen and lower body can occur due to fluid retention.
Many of the clinical features of chronic liver disease are related to the failure of the liver to carry out its normal functions.
Jaundice
Jaundice in adults is a yellow discoloration of the skin and whites of the eyes, which usually occurs when serum bilirubin is greater than 50µmol/L. Jaundice can occur with acute or chronic liver disease and does not give an indication of liver function.
Pale stools
Pale stools are a sign of biliary obstruction. Normally bile is secreted into the intestine where it is incorporated into the faeces, changing the colour. If there is biliary obstruction bile secretion is reduced, resulting in pale stools.
Dark urine
Because patients with biliary obstruction are unable to excrete water-soluble conjugated bilirubin via the faeces, the body compensates by increasing renal elimination of bilirubin. This darkens the colour of the
urine.
Spider naevi
Spider naevi are small vascular malformations (arterial-venous shunts) that occur in the skin and hands. They are not specific to liver disease, but may indicate impaired liver function. Palmar erythema (red palms of hands) also occurs commonly in chronic liver disease.
Bruising and bleeding
Patients with chronic liver disease often experience increased bleeding from the gums and mouth and easy bruising. This is primarily related to
abnormal clotting of blood caused by a reduced ability of the liver to synthesise clotting factors.
Encephalopathy
Hepatic encephalopathy (HE) is a neuropsychiatric syndrome that occurs in patients with significant liver dysfunction. Characteristics of HE include reduced concentration, confusion, changes in sleep pattern and asterixis (also know as the “hepatic flap”), which presents with hand tremor and inability to keep the wrists extended on outreached hands. The precise pathogenesis of HE is unknown, but it is widely accepted that this complex
syndrome results from the failure of the liver to remove gut-derived toxins[2].
It has also been suggested that patients with HE have an altered blood-brain barrier, which allows high levels of circulating systemic toxins to cross into the central nervous system.
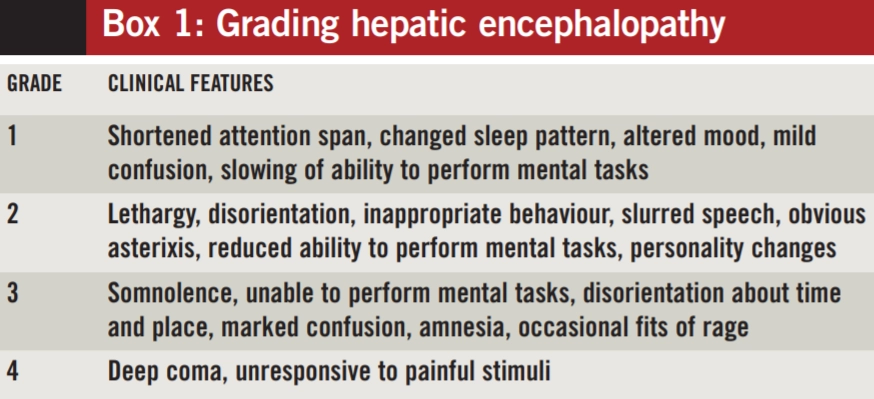
Ammonia, which is derived from protein breakdown in the gut, is usually metabolised in the liver to urea and has long been suspected to be the key toxin. However, it should be noted that there is a poor correlation between blood levels of ammonia and the severity of HE, suggesting an indirect effect[2]. Based on a patient’s clinical features, HE can be graded into four stages of increasing severity (see Box 1).
Portal hypertension
Portal hypertension is increased pressure within the portal venous system as a result of increased resistance to flow through the damaged liver; collateral veins develop and these can bleed due to the increased flow and pressure within (see “Varices” below).
Splenomegaly
Splenomegaly can be caused by increased pressure in the portal venous system and indicates portal hypertension secondary to cirrhosis.
Varices
Oesophageal and gastric varices are abnormally dilated collateral vessels in the oesophagus or stomach, which arise as a result of portal hypertension or obstruction. These varices enable blood to bypass the liver as a means of reducing the portal pressure or bypassing the obstruction. If the pressure in the vessels becomes too high they can burst, leading to massive haemorrhage.
Gynaecomastia
Gynaecomastia can occur in men with liver disease because of the inability of the cirrhotic liver to metabolise oestrogen; in women of reproductive age this effect on sex hormones can reduce fertility.
Pruritus
In chronic liver disease, high concentrations of bile salts can accumulate in the skin, causing itch. This is common in cholestatic conditions and can have a significant impact on patients’ quality of life.
Ascites
Ascites is the accumulation of excess fluid in the peritoneal cavity, leading to a swollen abdomen. Mild ascites is difficult to detect, unlike severe ascites, which causes abdominal distension. Ascites is the most common complication of liver cirrhosis. The formation of ascites is related primarily to an inability to excrete an adequate amount of sodium into urine leading to a positive sodium balance.
Patients with ascites generally complain of progressive abdominal heaviness and pressure in addition to shortness of breath caused by mechanical impingement on the diaphragm.
Evidence suggests that splanchnic vasodilation (caused by portal hypertension) decreases the effective blood volume leading to activation of the sympathetic nervous system and the renin-angiotensin-aldosterone system. This causes renal sodium and water retention and formation of ascites and oedema[3].
Patients with ascites generally complain of progressive abdominal heaviness and pressure in addition to shortness of breath caused by mechanical impingement on the diaphragm. Ascites can also be caused by conditions such as malnutrition and heart failure.
Assessment of liver function
Measuring albumin and prothrombin time is important when assessing hepatic function because they provide an indication of the synthetic function of the liver.
Assessment of liver function also includes conducting routine liver function tests (LFTs), which include:
- Bilirubin;
- Aspartate transaminase (AST);
- Alanine transaminase (ALT);
- Alkaline phosphatase (ALP);
- Gamma glutamyltransferase (GGT).
These markers provide a relatively crude measure of liver function. In general, serum elevations greater than twice the upper limit of normal are usually considered significant changes.
A detailed discussion of LFTs is outside the scope of this article, but can be found in an article previously published in Clinical Pharmacist (2009;1:363).
Liver ultrasound provides visualisation of the bile ducts and the texture of the liver and is used to exclude obstruction as a cause of liver dysfunction. It is also used to investigate for possible liver tumours and to assess the extent of splenomegaly and portal hypertension. Liver biopsy is used to assess the severity and nature of liver disease (eg, to differentiate between hepatitis and cirrhosis).
Child-Pugh classification
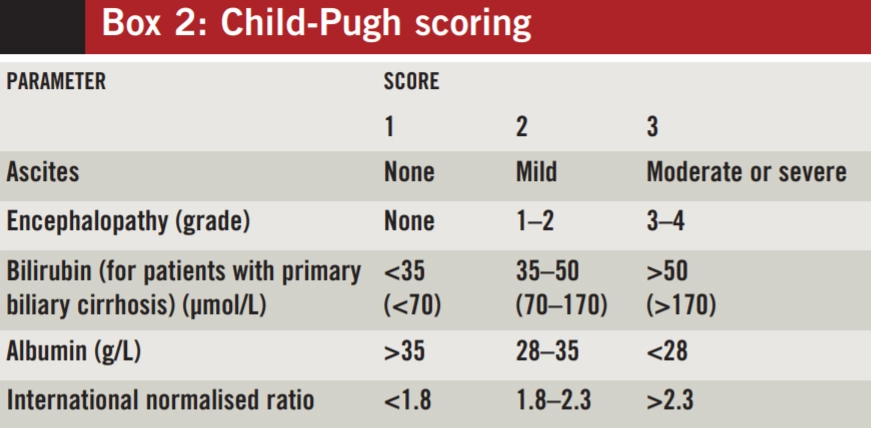
The Child-Pugh score is used to classify the severity of liver cirrhosis, from A (least severe) through to C (most severe). Five variables are considered — ascites, encephalopathy, serum albumin, bilirubin and blood clotting. Each variable is assigned a score between 1 and 3 according to the severity or degree of abnormality[5]. The sum of the five scores (see Box 2) is used to assign a grade of A (score £6), B (7–9) or C (³10).
Pharmaceutical manufacturers sometimes use the Child-Pugh grade to suggest dose reductions or to contraindicate the use of a drug. However, the use of this tool to guide drug dosing is limited because two patients with the same classification can have markedly different metabolic capacity. Therefore the Child-Pugh system should be used only to assess the severity of liver disease.
Model for end-stage liver disease
The model for end-stage liver disease (MELD) is a scoring system used to prioritise patients awaiting liver transplantation. Patients with a higher score are deemed to require a transplant more urgently than those with a lower score. Serum bilirubin, creatinine and INR are the parameters used to calculate a MELD score.
Acknowledgement: Thanks to Mark Thursz, professor of hepatology at Imperial College London and consultant in hepatology at Imperial College Healthcare NHS Trust, London, for his comments and review of the article.
References
- Griffiths C, Rooney C, Brock A. Leading causes of death in England and Wales — how should we group causes? Health statistics Quarterly 2005;28:6–17.
- McAvoy N, Hayes P. Hepatic encephalopathy. Medicine 2007:35:108–11.
- European Association for the Study of the Liver. EASL clinical practice guideline on the management of ascites, spontaneous bacterial peritonitis, and hepatorenal syndrome in cirrhosis. Journal of Hepatology 2010:53:397–417.
- Goodman ZD. Grading and staging systems for inflammation and fibrosis in chronic liver disease. Journal of Hepatology 2007;47:598–607.
- North-Lewis P (ed). Drugs and the liver. London: Pharmaceutical Press; 2008, pp97–8.


